

Welcome to The Ripple Effect – Hypnobirthing course. I do hope that this will inspire you and support you during your pregnancy, labour, birth and parenting journey. The tools you will develop are “tools for life” that are beneficial for you, your baby and your birth partner and any others that may support you during this amazing journey.
What we will focus on:
Session 1:
- Overview of course
Breathing and relaxation + Environment + Mindset = Positive Birth Experience
- What is Hypnosis?
- The subconscious and how it works
- Hypnosis Session 1
Session 2:
- Emotional stages of Labour
- What happens in Labour (overview of what contractions are doing and why we have them)
- Difference between ‘Fight-or-Flight’ and the ‘Relaxation Response’ and how that affects labour.
- The importance of the environment and creating your ‘Nest’
- Affirmations
- Hypnosis 2
Session 3
- Breathe Release Let Go
- Breathing together
- Massage
- Mind map
- Birth Video
- Hypnosis 3
- Summary – what to do now
Session 4
- Rebozo
- Basic Yoga flow
- Spinning babies techniques

“Hypnobirthing” is not a new concept.
Grantley Dick-Reid (1889-1959) wrote in his book ‘Childbirth without Fear’ that women who were not frightened about giving birth usually experienced a pain-free birth that did not necessitate any analgesics or strong pain medication.
Marie Mongan (pioneer in birth education with hypnosis), ‘developing’ the concept in The United States of America in 1989 (www.hypnobirthing-uk.com).
Many ‘leading’ hypnotherapists and birth practitioners have claimed their own methods. Each has it’s own merits and each will say theirs is the one that really makes the difference. The term ‘hypnobirthing’ is a set of tools and skills which can help and support the mother-to-be so that she has a clear perception and understanding of the journey ahead of her and the physiology of labour.
There have been various research trials over the years which have claimed using hypnosis for birth has led to:
- A reduction in length of labour
- Less reported pain
- A reduction in medical intervention and use of forceps or ventouse
- A reduced Caesarean rate
- A reduced need for pharmacological anaesthesia/analgesia
- Higher Apgar scores
An Apgar score is a visual assessment a midwife gives a baby once it is born.
It will be done at 1 minute after birth and then at 5 minutes after birth.
All of these findings would be expected in women who were calmer during birth regardless of whether they were using hypnobirthing or not.
Evidence Based Birth website, Rebecca Dekker mentions a couple of trials which support the above claims;
2016 Madden et al. published a Cochrane review and meta-analysis. The review included nine randomized, controlled trials with a total of nearly 3000 participants. They found , people who received hypnosis were 27% less likely to have any drugs for pain relief overall. This could have included epidurals, or injectable opioids, or nitrous oxide gas.
A study by Werner et al. published in 2013 was carried out in Denmark and it had 1,222 participants (the biggest trial included in the Cochrane review mentioned above) The people who were randomly assigned to hypnosis received three, one-hour training sessions and they were also given three audio tracks to listen to at home. The other group, the control group, received three, one-hour sessions on relaxation practices in which they learned techniques for relaxation, as well as mindfulness techniques. And the relaxation group also received audio tracks to listen to at home to help them with their relaxation practice. The researchers used a validated tool to measure fear, confidence, and expectations before the actual birth, and then they evaluated the same aspects of the childbirth experience six weeks postpartum. They found, women in the hypnosis group experienced their labours as significantly better on average compared with the other group.
All sounds good, but, unfortunately, nothing is hands down conclusive. We do, however, have lots of anecdotal evidence from couples who have used hypnobirthing in some form or another and those who have done a course (as opposed to having followed a video etc.) would state hypnobirthing made a positive difference to their birth experiences. It is also incredibly popular.
How does it help a woman give birth?
In theory women don’t need ‘help’ to give birth – we’ve been doing it since the beginning of time.
- There’s a long history of fear built up around childbirth, and a combination of that
- How birth is represented in modern society and the constant stream of horrific birth stories have made women very frightened.
Birth is a physiological function i.e. a subconscious element all female mammals are born with, along with the ability to breath; to digest food; to pump blood all the way around the body via the heart etc. It belongs in the realm of the ‘old brain’ the part we share with all other mammals. However, as ‘higher level intelligent’ mammals i.e. humans, we’ve developed the ‘new brain’ or Neocortex which is the part of the brain that deals with rational decisions, critical thinking and analysing amongst other things.
Women tend to approach childbirth from a very ‘Neocortex’ point of view, by planning and risk assessing. Whilst this is understandable, Ina May Gaskin points out you cannot think your baby out. Hypnosis for childbirth enables women to switch off the thinking part of their brain and allow the instinctive, mammalistic part to take control. It also enables us to relax both leading up to and during the birth which supports the physiological aspect of birth and allows the beneficial birthing hormones, Oxytocin and Endorphins to do their job without being cancelled out by the birth stopping Adrenalin. But in order to really understand how ‘hypnobirthing’ works, we have to look at how hypnosis works.
Why can hypnosis and a knowledge of the physiological process of labour make childbirth a truly empowering experience?
What is Hypnosis? A brief history
Different cultures around the world have used hypnosis in all its different guises for centuries. Different practitioners at different periods of time have experimented with its use to either wide acclaim or monumental disapproval. But whatever people’s feelings are about it, the use of hypnosis is a technique which has fascinated people since the beginning of time.
One of the most famous practitioners of hypnosis, and the first to try to understand the way it worked, was Franz Anton Mesmer (from whom we get the word ‘mesmerism’). He lived and worked during the 1700s and the basis of his work was on what he called animal magnetism.
He used magnets and iron rods placed in water to treat his patients and was into the drama and theatricality of it in a big way. However, because of this his theories were discredited and he spent the last three decades of his life living as a virtual recluse. However, others soon followed in his footsteps because they came to realise it wasn’t just the theatricals which brought about any healing, but the trance-like state people seemed to enter.
In the mid 1800’s, a doctor from Manchester, named James Braid created the word ‘hypnosis’ from the Greek God of Sleep – Hypnos, as he noticed, people in hypnosis appeared to be asleep when in a trance-like state. This is possibly what leads may people to think they will be put to sleep during hypnosis or they have been asleep whilst being hypnotised, despite that not being the case at all.
Meanwhile, Dr James Esdaile, a Scotsman working in India, was using hypnosis as a form of anaesthesia to perform a variety of minor and major surgical procedures. Even though these were successful, his work was (understandably) met with very little enthusiasm.
Dr John Elliotson, who was practising at the same sort of time as Esdaile, was the first to demonstrate the use of hypnosis in British Medicine. Again, despite the fact he had performed many successful operations whilst using hypnosis, his work was greeted with contempt (possibly because it undermined the science behind the medicine) and both his and Esdaile’s methods of hypnosis as anaesthesia were being replaced by the public’s preferred choice of chloroform.
Sigmund Freud (late 19th Century) held the belief that many problems (mental and physical) in adult life were due to unconsciously repressed memories and sexual desires, a lot of which featured unorthodox thoughts about one’s parents. This possibly presents a reason why people may have avoided hypnosis at that time as they did not want to be associated or have access to some quite disturbing thoughts!!
Milton Erickson was a hypnotherapist in Arizona during the 20th century. He can perhaps be credited as the person who made hypnotherapy more acceptable in western medicine and he used it in a wide range of situations, helping patients , other therapists had declared ‘incurable’. He pioneered the work in indirect and direct suggestion which most of our modern-day hypnosis scripts are based on.
But what actually is ‘hypnosis’?
What were all these people trying to achieve by using it and does it work?
The British Society of Clinical and Experimental Hypnosis describes it as follows:
“In therapy, hypnosis usually involves the person experiencing a sense of deep relaxation with their attention narrowed down, and focused on appropriate suggestions made by the therapist”
Hypnosis has been around for a long time. It has been used to develop creativity and to improve public performance; athletes and sports professionals have used it to improve their sporting abilities; sales people, trainers and managers use it to increase business success and there have been great advances with it in the field of medicine, psychology and pain management. There are over 11,000 research studies on hypnosis and hypnotherapy cited on PubMed – the world’s largest database on scientific research. Despite this, the General Public, tend to have very specific views on what they think hypnosis is or isn’t. There are those who have used it for therapeutic reasons such as dealing with phobias or anxieties, who will swear it is the best thing since sliced bread. There are those who have also used it for therapeutic reasons such as giving up smoking who have found it useless. There are those who see it as a form of entertainment!
However, thanks to scientific advancement, we do have an advantage over the earlier practitioners of hypnosis in we now have the ability to measure the electrical activity of the brain to identify what is happening in the brain whilst in different states. This has identified four main types of brain waves.
Beta Waves (15-40 cycles per second)
These are characteristic of an engaged and focused mind. A person taking part in active conversation would be in Beta rhythm as would someone teaching or debating.
Alpha Waves (9-14 cycles per second)
These are slower than the above and represent a less aroused state. For example, if we had been busy doing something complicated, we might sit down afterwards to have a rest and at this point we would go into Alpha rhythm, a more relaxed state of mind. Alpha waves are not present when we’re in a deep sleep, highly aroused or experiencing fear or anger, they are present at times of creativity or productive problem-solving and during lighter hypnosis and guided meditation.
Theta Waves (4-8 cycles per second)
These are present when we’re feeling very calm; in medium to deep hypnosis; dreaming and in some meditative states. Theta rhythm is associated with our subconscious mind where we hold all our past experiences, thought and behaviour patterns. You’ll have experienced this depth of brain wave activity on many occasions, daydreaming for example, or brushing your teeth as part of your daily routine. Ever experienced driving the car from A to B, arrived at B and not remembered doing the journey? That’s Theta rhythm. But if someone had jumped out in front of the car or you suddenly realised you had no idea where you were going, your brain would have automatically switched to Beta rhythm to drive safely. We often have good ideas on long or repetitive journeys or whilst doing some other familiar activity, because we’re not having to think about anything else, therefore we can mentally switch off and indulge in creativity.
Delta Waves (1-4 cycles per second)
These are produced in our subconscious mind and when we are in our slowest, deepest state of rest. This is a state of detached awareness, sleep and possibly representative of very deep hypnosis. Dreamless sleep will take you down to the lowest frequency of 2 or 3 cycles per second but never to zero as this is the state of being brain-dead! If brain scans of clients were taken during a hypnosis session, Alpha and Theta waves would be seen since these are the ones which enable access to the subconscious mind.
Accessing the subconscious mind is the basis of the success of hypnosis.
What Hypnosis is NOT is Mind control.
A lot of people are suspicious and concerned about being ‘placed’ in a trance state. For the majority of people, their experiences of hypnosis are centred around entertainment, films or fiction. If this is their only frame of reference then it would seem hypnosis is all about somebody else controlling them – telling them what to do and say – with them having very little choice about it. Understandably, this is a frightening concept as no-one likes the thought of letting somebody else control their mind. But the slowing down of our brain waves is, in fact, a very natural, normal occurrence and happens several times a day without us even realising it.
It is not something you can get trapped in – that is the stuff of fiction. If we’re in a naturally ‘hypnotic’ state, such as driving down that familiar stretch of road, and somebody in front of us suddenly stopped, we would snap out of that state and react accordingly. If we were daydreaming whilst brushing our teeth and our child called to us for help, we would naturally ‘come to’ and be able to respond. Nor is it a case of somebody else being able to control us, even in the case of a stage hypnotist. If the chosen member of the audience felt uncomfortable, with the hypnotist’s suggestions, for whatever reason, it wouldn’t work. The key to any hypnosis session is the subject is open to being hypnotised, whether that’s them wanting their 15 minutes of fame (despite knowing they are likely to be told to do something silly) or wanting results therapeutically. The perfect example of this is the person who saw a hypnotherapist to give up smoking and it didn’t work. The most likely reason it didn’t work is because the subject only went, because friends and family were begging him to. Unless he categorically wanted to give up himself, he wouldn’t have been open to the hypnosis.
Being in a hypnotic state quietens the conscious, analytical, rational, thinking part of the mind (the Neo-cortex) in order to gain direct communication with the subconscious, emotional part. It sounds odd, but we naturally dip in and out of these two parts of our mind hundreds of times a day, within a split second. Think about the differences between how you feel when you’re actively having to think about something and when you’re doing something which requires no thinking at all, such as scrolling through Facebook or Instagram?
There is constant communication between the two parts of our brains, but we’re not consciously aware or ‘in control’ of that communication. So much so that entering into a hypnotic state is a very natural normal part of everyday life – if we lived in a calm, non-pressurised society, we would naturally be in this state for roughly twenty minutes every hour and a half, as discovered in a study by American psychologist, Ernest Rossi in 2002 (Mednick et al). It is difficult to be specific about what it feels like to be in a hypnotic state because everybody experiences it differently, but when it happens, people generally feel:
- Deeply relaxed
- Very focused on one thing
- Their mind wanders
- A bit distanced from their actual surroundings
- That time passes in an illogical way
- Very open to positive suggestions
We know natural hypnosis is:
- Something that happens all the time when we’re awake, several times a day
- A communication between the two parts of our mind we’re not usually aware of that varies considerably depending on the depth and quality of the trance
What is intended hypnosis?
Intended hypnosis is putting oneself in a trance state on purpose, either through self-hypnosis or with guided instruction. It is re-creating the natural hypnotic state of every day to intentionally connect into the part of the mind responsible for all change – the subconscious. The subconscious, unlike the conscious mind, is totally receptive and, as long as the subject is willing and open to the suggested changes, they can’t be blocked by the rational, critical, analytical conscious mind. For this reason, suggestions are far more likely to succeed than if the subject was relying on willpower and determination alone.
Alman and Lambrou (1983) state:
“Hypnosis is a state of mind in which suggestions are acted upon much more powerfully than is possible under normal conditions. While in hypnosis, one suppresses the power of the conscious criticism. One’s focus of attention is narrower and one’s level of awareness on a focal point is much higher than if one were awake. During this heightened focus and awareness, suggestions appear to go directly into the subconscious… You can control areas yourself which are normally out of reach of your conscious mind.”
Again, it is important to stress, hypnosis is NOT something done to a person when under someone else’s control. A hypnotherapist (or hypnotist) may be able to guide a person with the use of words but it is completely up to them, which suggestions they choose to follow. When they are being taken through a visualisation – even if they are told they are at a beach or in a forest – they can decide whether to follow it or not. It is up to them where that beach is, or who’s there with them. They can even choose not to be on a beach or in a forest and go wherever their mind takes them, or they may just see colours and hear sounds. In the same way, if certain suggestions do not sit comfortably or they feel wrong or dangerous, then their subconscious mind will not accept those suggestions or take them on board. The difference between a ‘hypnotist’ and a ‘hypnotherapist’ is that one uses this state of mind (hypnosis) for entertainment and one uses it for therapeutic gain. The similarity between the ‘subjects’ is that in both cases they are open and willing to receive the suggestions. If someone does not want to be made to cluck like a chicken, no one can make them do it but if they want their fifteen minutes of fame then there are endless possibilities. By the way, it is worth mentioning that someone can be very susceptible to suggestion in a therapeutic session but hypnotic suggestions will not work on them in the context of entertainment.
So, what does it feel like when someone is deliberately put into a ‘trance’ state? Different people will experience different levels of trance depending on their openness to the situation. Often people will say it didn’t work on them but, more often than not, it is because they have to learn to trust the person guiding them and once they do, they will enter into a trance state more quickly and more deeply than on previous occasions.
It is also a very normal phenomenon for people to find their mind starts firing off random thoughts as they begin to enter into a deeper level of trance. Budha called this the monkey mind and it can help to know this might happen. If you find it happens when you start practicing, try to give your monkey mind something to do i.e. re-focus on the hypnotherapist’s voice, or focus on your own breathing or muscles relaxing.
Many people will start to feel very heavy as though they are sinking into the surface they are lying/sitting on or they may feel extremely light as though they are almost floating above themselves – this is due to the feelings of relaxation and the release of muscle tension.
When you start practicing with hypnosis, be reassured that you can move and change position as you see fit. And, if at any point you feel as though you want to come out of the trance state, all you need to do is to open your eyes – it is that simple. A lot of people feel, especially once they become used to the sensations, as though they are falling asleep. They are not asleep (although some people do snore!) they are simply very relaxed but the beauty about hypnosis is the subconscious is always listening and taking in the information despite not consciously being aware of what is being said. You’re also likely to notice a time distortion – sometimes your experience feels as though it has lasted ten minutes when the session has been twice that length or it may feel as though you have been ‘out’ for ages when the session was only twenty minutes. What is happening as the trance deepens is your generalised reality orientation (GRO) is fading. The Generalised Reality Orientation One of the main reasons childhood is such a time of wonder is that children are constantly experiencing new events they have never experienced before, each one totally new. As we grow up we assimilate new situations and develop a frame of reference, a world view, a belief system, a map – in other words our Generalised Reality Orientation (GRO). A sort of filing cabinet where we can access thoughts or experiences to help us make sense of the world around us. This helps us, for instance, to recognize a movie is not real life, because we have a context in which we know the movie is just a movie. It helps us to know chocolate is tasty and spinach, perhaps less so because of the circumstances in which we were first introduced to these foods. As we get older and are less likely to come across totally unique experiences, any new events that happen are either slotted into pre-formed categories or are rejected as irrelevant. However, it is these frames of reference, whether they be in the form of memories, fears, beliefs and patterns of behaviour, that can dictate how we respond to certain situations or incidents no matter how inappropriate they may be e.g. running away from a spider or being frightened of flying (or even being scared of giving birth.). One of the main things that happens in hypnosis is that our GRO fades and the more it fades, the deeper the trance and the more our critical faculties reduce i.e. we become more open to the positive suggestions the hypnotherapist puts to us without feeling the need to disagree or access our past experiences to prove why things won’t/can’t happen the way it’s being suggested. Therefore, using the state of hypnosis to make changes can be so much more effective than just being given direction which needs to be processed consciously. It is also why it’s so much more effective than willpower.
So, to summarise:
- Hypnosis is a pleasant, natural state of mental relaxation with no negative side effects.
- It is not the same as being asleep or unconscious, even though in deeper states of relaxation it may feel like that, and people are always under their own control, no-one can make anybody do anything they don’t want to do.
- It is a communication between two levels of the mind and happens all the time when we’re awake, even though it is not something we’re usually aware of.
- This communication is even more enhanced when intense emotion of either a positive or negative nature is experienced.
- Intended hypnosis is making use of the above, to achieve a desired result or change.
The Subconscious 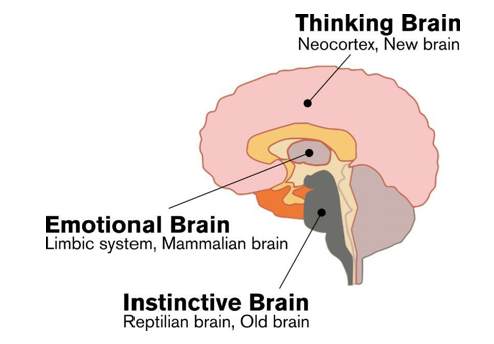
For us to fully understand how hypnosis relates to the subconscious and the significance of that, we need to understand how the brain works.
The Neocortex is our ‘thinking brain’ or conscious brain and it is this, which separates us from all other mammals on the planet. We’re still mammals and share other parts of the brain such as the limbic brain ‘emotional brain’ and the Reptilian brain or ‘instinctive brain’ but the Neocortex is what makes us mammals of higher intelligence and what enables us to walk upright and talk.
The Neocortex has enabled us to ask questions, solve problems, invent, create, plan, think etc. etc. but because of its ability to analyse, it also enables us to ask ‘What if?’ This creates fears, causes us to attach emotional significance to events and concepts and to catastrophise which gets in the way of many physiological (old brain) processes.
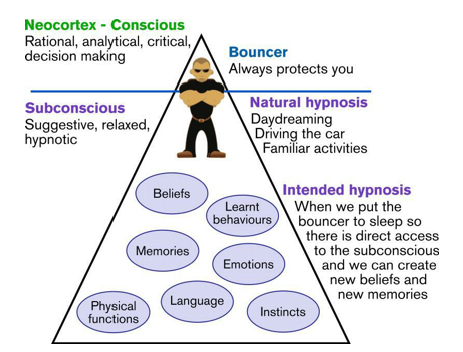
If you imagine the mind as a triangle. Only the very tip of it is the conscious brain (or Neocortex). The rest of it is taken up by the subconscious, the part of our mind which stores all the information it is given and everything it experiences. It’s very literal, doesn’t understand nuances or hints, and its primary task is our survival, therefore, it will nearly always win over the conscious mind. When a baby is born, the subconscious is pretty much a blank canvas because their ‘Generalised Reality Orientation’ (which we mentioned in the last chapter) develops as they grow up. In other words, everything else gets ‘put’ there by various means as the baby develops and learns. However, regardless of a developing GRO or not, a baby is born with instincts (to cry; to search for food etc.) and physical functions (breathing; pooing and weeing; heart beating etc.) – in other words the elements which are necessary for survival, the elements they share with all other baby mammals on the planet, are already there as soon as the baby is born. It is also worth noting all female mammals (including us!!) are born with the physiological function/ability to give birth to their young.
Beliefs
As we grow, we’re exposed to many types of belief structures ranging from believing blue is the colour blue; to how to behave in public; to what religion we follow (or not) and what practices we do or don’t take part in. We’re influenced by our parents, our society, our culture, our generation. We receive information from television, the internet, our teachers and figures of authority, to name but a few.
There is overwhelming support for certain belief systems and overwhelming criticism for others depending on where and when you grew up.

Think about some of the things you inherently believe – maybe it is to do with birth, maybe it’s something to do with your beliefs in yourself. Can you pinpoint exactly where they came from or are they simply a part of what makes you, you?
Memories
Every experience gets stored in our subconscious in the form of memories. Some we can easily, consciously remember just by casting our minds back. Some are triggered by a song (ever caught yourself singing along, word perfect, to a song on the radio you last heard 20 years ago?) or a photograph or a certain smell. But there are some memories our subconscious has kept hidden – maybe because they are considered too insignificant or because they are so significant, it would be ‘dangerous’ for us to remember the actual event. This is often (although not always) the cause of phobias and anxieties.
Emotions
These are part learnt and part instinctive. In other words, we’ll have a natural instinct to feel a particular emotion connected with a particular situation or incident but a lot of the time our parents/ teachers/ people around us will let us know whether that emotion is ‘acceptable’ or not. For instance, if a baby falls over it’s more often the parents’ reaction that tells him to cry or not. Or, if a parent is scared of dogs or spiders or flying, for example, it’s often the way they behave when exposed to those triggers that inform the child they need to be frightened too. Ever been told not to cry when it was a completely instinctive response to what you were feeling at the time?
Emotions also tie in with language.
Words can become so much more significant when we can attach emotion to them, the word ‘risk’ for example becomes so much more of an issue when there are emotional factors at stake. So if you were told there was a ‘risk’ you could fall of the pavement and twist your ankle you’d be less emotionally stimulated than if you were told there was a risk your baby.
Learnt Behaviours
When we learn to do something, we process it consciously. Once it’s learnt and is something we do on a regular basis, we no longer need to think about it because it’s stored subconsciously. Driving is the best example – at first the process requires a lot of thinking. Once you have passed your test and you drive regularly, the process becomes automatic and you simply put your key in the ignition and off you go.
However, there are, in fact, several stages of learning we have to go through before behaviour can become automatic:
Stage 1 – Unconscious Incompetence.
We’re not even aware of a particular ‘skill’ and have no idea how to do it. (Being a child passenger in the back of your parents’ car)
Stage 2 – Conscious Incompetence.
We’re now aware of it, want to do it, but have no idea how to go about it. (Our first few driving lessons and trying to co-ordinate ‘mirror, signal, manouvre’ with having three peddles and only two feet!)
Stage 3 – Conscious Competence.
Now we can do it, but we really need to concentrate, focus and think through the process. (Probably ready to take our test by this stage, but it is so necessary to concentrate)
Stage 4 – Unconscious Competence.
It is now so familiar to us it requires no thinking, our subconscious takes over and we go through the process automatically. (Once we’ve been driving for a while) Once we’ve reached the state of Unconscious competence, our behaviours have been learnt and they can be consigned to the subconscious. We have to store behaviours this way because otherwise it would take us a long time to re-learn and work our way through a process every time we went to do it.
Language
Language is all in the subconscious. From the moment a baby is born they copy the sounds they hear from their parents. All the ‘oohs’ and ‘ahhs’ is them mimicking the noises they hear and when a parent repeats it back to them it reaffirms that these sounds are good sounds to be making. If parents are bi or multi-lingual, then this is the best time to teach them other languages – a baby will pick it up so much quicker than waiting until languages are taught at school. However, as well as emotions, language also feeds into our belief systems, and gives ‘direction’ on how something is viewed.
For example; a woman in a position of power is often described as ‘cunning’ and ‘manipulative’ but if she was referred to as ‘clever’, then it puts a very different emphasis on the situation. A student could be labelled ‘argumentative’ and ‘obstructive’ or he could be identified as ‘intelligent’ and ‘questioning’. It’s very difficult to change all of these pre-existing and, in many cases, long standing beliefs and behaviours etc., just by talking to a conscious mind. By using intended hypnosis we’re able to create new beliefs and memories and better responses to emotional triggers in the future because hypnosis allows access to the subconscious when all our frames of reference have been temporarily removed so it is much easier to make changes. This is done via the use of post-hypnotic suggestions.
Post-Hypnotic Suggestions
Every action has a reaction – if we’re hungry, we eat; if we’re thirsty, we drink; if we’re stressed, we might bite our nails and so on. So much of our unwanted behaviour is down to triggered responses based on our past experiences. On a conscious level, we may not even be aware of why we do certain things or why we have certain responses to a particular object or situation, which is why we may find habits, phobias, addictions etc. so hard to break or change. However, by using hypnosis, we can re-train the mind and create new and better responses to the trigger in the future, as long as the new responses are beneficial to us.
Hypnosis scripts are the method by which a person is taken into an intended hypnotic state and within that script will be two types of suggestions. There are direct hypnotic suggestions which are related to the things you’re told to do during a hypnosis session, making it more likely it will be a success, such as “close your eyes”, “focus on your breathing” etc.
There will be post-hypnotic suggestions, the ‘magic’ behind hypnosis, and what makes it different from other relaxation techniques such as mindfulness and meditation. They work on the basis that when you’re faced with the situation currently making you anxious, you’re unlikely to be lying down in a trance-like state, so a post-hypnotic suggestion is one given to a person whilst in a hypnotic trance, for an action or response to take place in the future after the hypnotic experience has ended. Anything which would have previously caused anxiety is re-worded into a positive trigger that can promote calm and relaxation. The more these post-hypnotic suggestions are heard, the more the mind accepts them as reality. In fact, the brain will create new neural pathways to show this new (and preferred response) has become learnt behaviour. So, when faced with the situation which was previously causing distress, we don’t have to think what to do to make ourselves feel better, it will just happen automatically, i.e. we’ve reached the state of unconscious competence.
The Importance of Relaxation
Humans are amazing (in fact all mammals) are. We have a very responsive and necessary life-saving reflex which is our Fight or Flight Response – the Sympathetic Nervous System.
This is ‘old brain’ stuff, instinctive and primal and stems from a time when we could afford to miss lunch but we couldn’t afford to be lunch!
The Relaxation Response or Parasympathetic Nervous System, also part of the old brain, also instinctive and primal is the direct opposite to fight or flight. The interesting thing is, we cannot be both – we’re either stressed or relaxed. It is either safe to be where we are or it isn’t – Remember the subconscious has no ‘maybes’, ‘ifs’ or ‘buts’. Imagine, a caveman skipping out of his cave only to be confronted by a sabre-toothed tiger.
The fight or flight response is triggered
- Adrenalin and Cortisol are released into his blood stream and the caveman is able to fight or run away from danger.
- His heart beats faster to drive the blood flow into his extremities to give his limbs more power where the muscle tension has also increased.
- His breathing has become shallower to accommodate the fact he is likely to be moving very quickly.
- He is also going to be hyper alert in case any other danger should present itself.
The very next day, he doesn’t wake up and skip to the door of his cave having forgotten all about the events of yesterday, the ‘fight or flight’ response kicks in and Adrenalin starts surging around his body even before he gets there, just in case.
In today’s society anything we perceive as not OK represents a threat to our subconscious and is going to produce exactly the same fight or flight response.
The relaxation response does the opposite.
- The heart rate is calm and steady and drives blood flow to all the muscle groups.
- Muscles are relaxed and not holding on to any unnecessary tension.
- Breathing has slowed right down and the breaths are longer and deeper.
- The focus is also much more internal because of no longer being under threat.
- This state is a much healthier one to be in for the long-term because all our internal organs work better when we’re in a relaxed state.
Being in a hypnotic state and the processes which we need to employ to get into that state, such as focussing on our breathing, relaxing our muscles etc. triggers the relaxation response which has both short-term and long-term benefits for life in general.
Hypnobirthing and The Subconscious
Everything is relevant to helping you prepare to give birth because, in the vast majority of cases, people approach this time of their lives surrounded by fear. More often than not, it’s fear that’s been embedded from way before you were even thinking about having a baby.
Beliefs, memories and emotions
Being or putting someone in a hypnotic state allows direct access to the subconscious, new beliefs and memories relating too birth can be created. As mentioned birth is viewed as dangerous and frightening by society.
Every time a birth is portrayed on TV or on a film it is accompanied by lots of people screaming. Women are shown in incredible pain, usually on their backs with legs in stirrups, and something usually goes wrong.
Our birth education should start in school where we have an opportunity to show birth as this amazing journey and contribute to our beliefs about birth. For those of you that follow my instagram account know that I share video clips which show gentle, calm births. Having taught Personal and Health Education in a school setting the curriculum is rather limited and with thought this could be developed to be so much more.
When we receive negative messages they stay in our subconscious, confirming and compounding the belief that birth is a frightening prospect. How your parents talk about their experiences when they gave birth to you also contributes to how you perceive childbirth – even if it is just a throw away comment about how many hours they were in labour.
Society reinforces that birth is painful and traumatic therefore encouraging women to ‘fix it quick’ – assuming that women will choose pain relief to give birth. We would have an anaesthetic to have a tooth pulled, why not when YOU are having a baby? Why would women want to crawl around on all fours when giving birth, when they could be nicely and decently tucked up in bed? It may be you are not even aware of how you feel about birth until you became pregnant and the impending realisation this baby has to get out somehow, becomes unavoidable. If fear and anxiety are the leading beliefs embedded in your subconscious, then you’re going to pick up on every single negative story from your friends or strangers you meet in the supermarket, in the newspaper and on television increasing your fear more and more on a daily basis.
Hypnobirthing can change those beliefs and create more positive ‘memories’ associated with birth (remember the subconscious is just going to accept the suggestions because in a hypnotic state, conscious criticism is quietened down) and because the subconscious is now primed to notice positive stories and images this in turn will increase your confidence in your ability to give birth.
Learnt behaviours
Many are scared about the pain of contractions and your default response would be to tense up, every time you feel one starting. The post-hypnotic suggestions we talked about earlier create a more positive response to contractions enabling you to work with your contractions rather than suffering from them. In fact any potential anxiety making ‘trigger’ can be given as a positive post-hypnotic suggestion i.e. “with each new face you see, you’re reminded to focus on your relaxation”, “on the journey from home to hospital, you focus on your breathing to take you even deeper into calm and focused relaxation”, “every time you feel your birth partner’s touch, it reminds you of how safe and protected you are”.
In your hypnotic state, these suggestions bypass the conscious mind and are stored directly as learnt behaviours. Therefore, when you go into labour, you won’t have to ‘think’ what you should be doing; your responses to the contractions will become automatic.
Language
Midwives and doctors will talk about what women are allowed to do regarding the births of their babies, which can make many feel as though they have to ask permission. Medical staff will also refer to themselves as delivering the babies which puts the emphasis on them as opposed to the mother. In my humble opinion, the only things that get delivered should be online shopping and take-aways! The types of interaction a mother has during her pregnancy and labour can, and does, affect her state of mind, which in turn affects her thoughts and emotions. This is very true when it comes to the mother’s perception of pain. How the contractions are presented and talked about can leave her interpreting her pain as manageable and productive or scary and threatening.
I honestly believe midwifery and medical training has no concept of how powerful and influential the words they use can be. This is where hypnobirthing comes in because the language used in hypnosis scripts is positive and empowering, e.g. we talk about you birthing your baby and being powerful and confident as you do so. It puts the emphasis on your body and your baby and encourages you to trust your instincts.
It also instils the importance of asking questions and making decisions based on information that concerns you as an individual rather than getting caught up in policies and protocols. It is important you and your partner feel as though you have been an active participant in any decision making rather than being pushed and pulled in directions you do not want to go.
Hypnobirthing and the Physiology of Birth
Being in a relaxed state, triggers the relaxation response, hypnosis supports the physiology of birth.
How does the presence of Adrenalin make labour harder and more painful than it needs to be?
Remember our caveman and how the fight or flight response made his heart beat faster to drive blood flow into his extremities, caused his muscles to tense, his breathing to become shallow and his mind to become super alert?
Now imagine if this was a cavewoman in labour.
- A faster heartbeat increases blood pressure which means she is more likely to lose too much blood i.e. haemorrhage, especially as the placenta starts to separate.
- In addition, blood flow directed towards the extremities i.e. away from the uterus, means this vital muscle is being deprived of fuel and it is going to run out of energy far quicker than is ideal.
- Muscle tension, which is so necessary to fight or run away from the sabre-toothed tiger, is causing her to hold herself rigid and the stomach muscles, which separate during pregnancy, are creating a wall of tension either side of the uterus. This means as the uterus contracts, it needs to fight the tension of the surrounding muscles, causing the contractions to be much more painful than they need to be.
- Shallow breathing which would be necessary if the cavewoman was moving quickly, is depriving the uterus of oxygen because the breath is not getting deep enough to fuel it. This means toxins such as lactic acid will build up in the uterus making the muscle feel crampy and even more painful.
- The uterus will also tire much earlier and cease to be efficient and of course the baby is not getting the oxygen he or she needs.
- She is hyper alert, looking for any further danger – again, this is positive when running away from something that can kill you, but detrimental to the birthing process because it floods her system with more and more adrenaline, making labour increasingly and consistently more painful.
- Her jaw is tense and tight because of muscle tension but this has a knock-on effect on the cervix – generally, if the jaw is tight so is the cervix.
- She could also be screaming, increasing her fear, and that of those around her and consequently wasting a lot of energy, hers and everyone else’s.
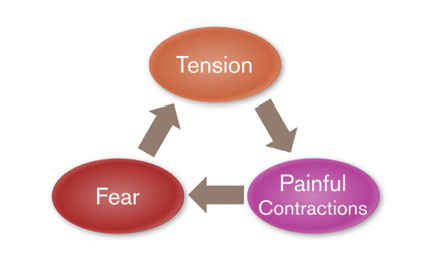
- She has got herself caught up in what we call the fear-tension-pain cycle. The pregnant woman is frightened, causing tension in the muscles, which makes the contractions more painful than they need to be.
- This cycle also causes labour to slow down or stop completely – a physiological reaction which makes sense from a mammalistic/primitive brain point of view:
- If the mother is in danger, it makes no sense for her baby to be born into that danger too.
- The slowing down or stopping of labour is due to Adrenalin flooding her system which causes the cervix to close, therefore minimising the risk of her baby being born into danger.
- She can then fight or run-away from the perceived predator, enabling both herself and her baby to get away from danger. Once she had reached a place of safety, the Adrenalin would leave her body and the birthing hormones would start to do their job again.
- Remember, anything a birthing woman perceives as not ok (cold, loud noises, strange environment etc.) is going to perceived subconsciously as a predator producing exactly the same effect as if a sabre-toothed tiger was standing in front of her.
In modern birthing society, if labour slows down due to the above cycle, she is likely to have her labour augmented (speeded up chemically) or she may be sent for a Caesarean.
In these cases, she may see the initials ‘F.T.P.’ written in her notes.
‘F.T.P.’ means ‘Failure To Progress’ – it’s not a coincidence that these initials are exactly the same as ‘Fear, Tension, Pain’.
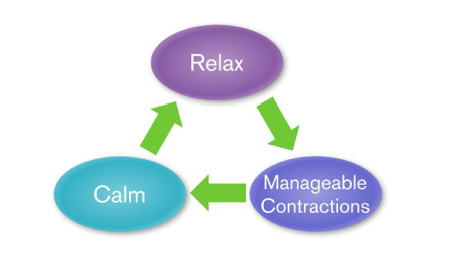
Now, if our labouring cavewoman was under the influence of the relaxation response which she would be if she felt safe and in no danger from any predator:
Her heartbeat would be regular and calm, meaning she is less likely to lose more than the normal amounts of blood after the baby is born (usually about 500 ml.) and because she is calm, all the blood flow is directed to the uterus, this fuels the muscle and keeps it going for as long as it needs.
Her muscles are loose and relaxed. This means she can also move and rock and sway with the contractions, helping the baby to negotiate the pelvis and move its way into the birth canal.
The repetitive movement encourages the release of Oxytocin and Endorphins (labour hormones), helps relax the mother even more and deepen the naturally hypnotic state she gets herself into.
Relaxed muscles also mean relaxed stomach muscles, so as the uterus contracts it does not have to fight against any additional tension, making each contraction far more comfortable and manageable.
Being so relaxed means that she is in a hypnotic state, she is breathing deeply and slowly which means the uterus has all the oxygen it needs to keep working efficiently and energetically, allowing any toxins to be flushed out of her system – again making contractions more manageable.
The baby is also getting plenty of oxygen which helps it copes with the physical effects of labour on its system more positively.
The natural hypnotic state induced by relaxation allows her to focus internally on what her body and her baby are doing, meaning she will instinctively and intuitively be responding to what her body is telling her to do and therefore she will become more and more deeply relaxed and focussed.
Her jaw is loose, reflecting the opening cervix and any noises she makes will be low, directing the energy where it needs to be.
The relaxation cycle i.e. the para-sympathetic nervous system or relaxation response, is a much calmer, positive and effective place to be in for labour.
Through the use of hypnosis and the post hypnotic suggestions, we can remove (or at the very least, massively reduce) any fear that may have been felt about childbirth before going into labour.
We can direct your attention to positive stories, increasing your confidence in your body’s ability to give birth.
We can also ensure your calm response to contractions, to changes of environment, even to changes of birth circumstances, becomes learnt behaviour and automatic.
A note on ‘the breathing’ as mentioned previously, there are various hypnobirthing methods in the public domain. Many of them refer to specific types of breathing, depending on where a woman is in her contraction.
Let’s keep this SIMPLE – you have been breathing since you arrived earth side and YOUR breathing changes according to what you’re doing – again this happens automatically. To give a physiological function specific steps, gives you something to ‘think’ about which makes the process very cerebral. Birth requires you to be responsive and instinctive – thinking will bring you back into the realm of the neo-cortex which is exactly where you don’t want to be. You can become confused as to what type of breathing you should be doing and this can lead to panic in a state of heightened emotion, causing Adrenalin to rush in and making labour harder work than it needs to be. I encourage my clients just to focus on their breathing, it does not matter whether they are breathing in and out through their mouths or their noses, they should just do what comes naturally. Focusing on the process of breathing naturally causes their breath to slow down and become deeper. If you find you need a little extra help the emphasis should be on the out breath.
“If in doubt….breathe out!”
When in a state of panic, we tend to breathe in shorter, sharper breaths and ever more rapidly, perversely making it harder and harder to take in any oxygen. By encouraging you to direct your attention to breathing out, your shoulders drop, your muscles relax and the relaxation response is triggered – simple! Muscle tension is released, carbon dioxide is expelled and the muscles tend to relax even more during this part of the breathing cycle. By focusing on breathing out for as long as possible (note, not necessarily counting although you can do that if you find it helps) the in-breath will naturally take care of itself and go as deep as it needs to (a fact that is very reassuring to a pregnant woman whose lung capacity is restricted due to the growing uterus.) This technique is also very useful to remember if you find themselves in an adrenalised state for whatever reason. Breathing out a few times can re-set the balance and help take you out of the ‘Fear, Tension, Pain’ cycle. Focussing on the breath is one of the methods used in hypnosis to take a person into a hypnotic state. It can also be used as a method of self-hypnosis.
A note on ‘the pain of contractions’
The word ‘pain’ is controversial amongst the hypnobirthing community – as is the word ‘contractions’.
Pain obviously has negative connotations because it is the body’s way of communicating there’s something wrong. It is also something that is feared because pain causes suffering and the thought of pain for a prolonged period of time, is frightening.
For that reason, many practitioners omit the word ‘pain’ from hypnosis scripts and in conversation about the process. This is also based on a story Grantley Dick-Reid tells in his book Childbirth Without Fear where he attended the birth of an impoverished woman who appeared to give birth without showing any signs of pain. When he asked her afterwards why it hadn’t hurt her, she replied she hadn’t realised it was supposed to. This formed the basis of his work, the idea that fearing the pain makes the whole process far more painful than it needs to be – remove the fear and you remove the pain.
Many hypnobirthing practices continue to teach this and feel if they don’t use the word ‘pain’ (and substituting ‘pressure’ or ‘power’) then clients won’t be tempted to think about it. In the same vein, there is a belief the word ‘contraction’ also has a negative connotation, that it is too closely connected with the idea of pain and prefer to use words such as ‘surges’ or ‘waves’.
Whilst this undoubtedly works for a lot of women, and various sources on the internet claim up to 1% of women say they have a painless birth, I have always been wary of claiming if hypnobirthing is practised properly and used correctly it will make labour completely pain free. Whilst it is fact that relaxing throughout a contraction will make it far easier to manage and less painful than if the mother were tensing up, for the reasons explained above, I fear the idea of a pain free birth could potentially cause more problems than it solves. The fact of the matter is, whilst some woman rightfully claim to have had a painless birth, the majority of women will feel their contractions. The more established labour becomes, the more intense the contractions, and yes, there are points during the labour that a mother may describe her contractions as painful. But that’s OK. Contractions should be felt because they serve a very useful purpose. They let you know where you are in the process – in other words, do you have time to finish gathering the wood and berries for the cave (shopping in a supermarket in modern day!) or do you need to hunker down and make sure you’re in a safe environment because this baby is coming?: They encourage you into beneficial, birth promoting positions – There is a reason most women find labouring on their back to be much more painful than when they are upright and leaning forward, because, quite simply, it goes against gravity:
It is a vitally important communication system – when you experience a contraction it provides hormonal feedback to the pituitary gland in the brain to provide more Oxytocin and Endorphins to progress the labour. There is evidence to suggest the amount of pain felt by a labouring mother depends very much on her perception of the pain. According to Rebecca Decker from www.evidencebasedbirth.com (2018), an Australian study, published in 2017 found that when mother’s interpreted their pain as productive and having a purpose and a normal part of the process – they were able to cope much better with the contractions than the women who interpreted the sensations they were feeling as threatening and frightening and felt medical help was necessary to relieve the pain.
They found there were two distinct states of mind that women might experience during labour – Mindful Acceptance where a woman was focused on staying in the present moment and made statements such as ”When a contraction had finished, I wasn’t worrying about the next one” or “I lost sense of time”, and Distracted and Distraught which was linked to higher levels of pain. These women would have said “I was looking at the clock and It just felt like every minute was an hour” or “I was dreading the next contraction” or “I was distracted by the people in the room”. So there is definitely room for re-framing the concept of pain. Unlike the pain from an injury, the strong physical sensation that you experience during labour is because a large muscle, i.e. the uterus is working hard. The sensation of the muscle working (i.e. contracting) is a positive one because it is bringing the baby closer to meeting you. But claiming labour can be pain free often means women may panic when they feel the intense sensations. If they start to panic, too much Adrenaline is introduced into the mix and labour becomes more stressful than it needs to be. We also have to be highly aware of how our social and cultural environments can greatly influence The Nocebo Effect. The Placebo Effect anticipates a good outcome so therefore that is generally what is achieved, but the Nocebo effect leads us to anticipate a bad outcome which is, consequently, usually then experienced. In terms of labour, certainly in particular parts of the world, there is so much cultural and social focus on the pain of childbirth, inevitably, that’s what women end up experiencing. Caregivers, really need to think about the way they present the topic of the pain of labour. Think about, for example, when women are told they will need an epidural if they are being induced because they won’t be able to cope with the pain of the contractions!! We can see when, culturally, birth is interpreted as manageable and productive, pain is not considered that big a deal. In the Netherlands, for example, only about 22% of women give birth with an epidural compared with 61% in the USA. Interestingly, what is clear and researched based is there are a lot of different factors that can influence how pain is perceived during labour. Environmental stressors, for example, such as over-crowded rooms, bright lights and restricted movements and the mother’s relationship (as in does she feel supported) with her caregivers – partners as well as midwives! – all contribute to a perception of increased pain. Hypnobirthing is the perfect antidote to all of this because it will help you to work with your contractions by using positive post-hypnotic suggestions, complementing birth physiology and encouraging the relaxation response through the use of specific hypnosis and self-hypnosis techniques, discussed later in the book. If you are still concerned about how much pain you’ll be in and how long it will last, then Milli Hill (founder of The Positive Birth Movement) sums it up perfectly in her book The Positive Birth Book (2017) by patiently working out that for an eight hour first stage of labour there are only 111 minutes of contractions which means a woman is only actually actually in ‘pain’ for 23% of her labour – the other 369 minutes or 77% of labour is entirely pain free!
The layout of a hypnosis script
As mentioned previously, anyone can enter into hypnosis, as long as they want to, and it is beneficial for anybody who does so. When attending a structured hypnosis session, or listening to a download yourself, you might find you enter into a relaxed state easily or you may find it really hard to switch off at first. Either is absolutely fine – remember as you get more used to it, your bouncer (he/she who protects the subconscious) will start to trust the process and you’ll find the process easier and easier each time you do it.
A hypnosis session will usually follow these steps:
- Setting the scene
- Induction
- Breathing and physical relaxation
- Deepener – guided imagery and visualisation
- Hypnotic/therapeutic suggestions
- Reorientation and exit
Setting the scene
You’re unlikely to be able to relax if you know you may be disturbed at any moment, so choose a time in your day when you’re not expecting any visitors or any deliveries. It is best not to do it when you’re getting into bed at night, simply because if you’re in your pj’s and lying under your duvet your subconscious is primed to send you to sleep.
Ideally you’d listen to the hypnosis tracks 2-3 times a week, leading up to every day in the last couple of weeks of your pregnancy.
Obviously if you’re working or you have existing children to take care of, finding time can be a bit trickier and if bedtime is the only time you can do it, then it is better than nothing – maybe try lying on top of the duvet though, instead of underneath it.
Turn your phones off, people can easily ignore other people’s phones but it’s hard to ignore your own.
Wear clothes you’re comfy in and that are not going to be restrictive – yes, technically you can do this wherever you are but you might as well stack the odds on your favour and make yourself as comfortable as possible.
Have somewhere you can lean or rest your head, pillows or cushions to support your bump if you’re lying down and something warm to cover your feet – or at the very least, wear socks.
It is so important to remember whatever you experience is absolutely fine, there is no wrong or right to this process.
Hypnosis is not about achieving an empty mind and if you do get random thoughts flying in and out just re-direct your attention to the words you’re listening to, or your breathing etc.
You can also change position throughout the session if you choose – there is nothing worse than forcing yourself to remain still even though you’re uncomfortable.
Remember as long as you’re open to doing the sessions and achieving positive change, hypnosis will work.
Induction
This is the process by which the ‘hypnotisee’ is guided away from their active conscious state and into a relaxed/suggestive/hypnotic state. It helps to slowly and steadily change their focus from the here and now reality, to the more internal focused state.
The most common methods are to focus on breathing or on muscles relaxing.
An example of an induction is as follows:
So, with your eyes comfortably closed, focus all your thoughts and attention on your breathing. Take a moment to be really aware of how it feels as, in your own time, you breathe in … and breathe out. [it can really help, if you’re writing it yourself to have someone else read it to you, to match this instruction with your natural breathing rhythm] Focus all your thoughts and attention on the sensation of air filling your lungs and then releasing. Imagine, with each breath in, you’re creating a sense of comfort… and on each breath out, you’re releasing any stresses, any tension and any anxieties you may be holding on to. You may like to imagine that every time you breathe in, your breath has a soothing, warm, colour which flows down and around your body … And every time you breathe out, that colour changes as you let go … … as you release all the stresses, tensions and any concerns… It’s as if, with each breath, you’re giving your body and mind permission to begin to let go, to begin to become more and more relaxed. Each breath becomes a trigger for your muscles to become soft and loose, for any tension to melt away, for your body to benefit from deep relaxation… Imagine with each breath, your muscles are becoming, softer… more and more supple… loose. With each breath, you take yourself even deeper into hypnosis… becoming more… and more… relaxed. Deeper and deeper into hypnosis… deep down… so safe… so comfortable. And the sound of my voice becomes the most important sound you hear… all other sounds, either from inside or outside of the room will simply fade into insignificance or help you to relax even more deeply. It’s my voice which is more and more comforting to you… more and more soothing to you. If any thoughts, feelings or images enter your mind…then acknowledge them, and then return your attention to the sound of my voice… this is your time… a time just for you, to enjoy as you choose… releasing and letting go more and more with each breath you take.
There are such things as rapid induction techniques which stage hypnotists would use and perhaps a hypnotherapist might use when treating a client on a regular basis to save time. However, for the purpose of hypnosis for childbirth, the process of relaxation and being aware of how it feels to enter the that relaxed state, is an extremely powerful technique and tool for you to learn to use.
Breathing and physical relaxation
A key element to any hypnosis session is breathing.
Slow, deep, rhythmic breathing triggers the relaxation response which sets off a chain reaction of physical changes.
Focussing on the out breath is the key to this.
So giving your in-breath and out-breath a specific colour can help you to focus as can imagining blowing out a golden thread or keeping a feather afloat.
Another element is relaxing the muscles – muscles work on an all or nothing principle, as discovered by Dr Edmond Jacobsen in 1929.
He found a large number of his patients had become so used to being in a constant state of muscle tension that they had become used to it. He realised if a patient consciously tensed and then relaxed a muscle, the muscle would be able to stay in that relaxed state. This process is called Progressive Muscle Relaxation or PMR and, whilst it is not necessarily used in all hypnosis scripts, relaxed muscles are very important during childbirth, so it is extremely relevant in the context of hypnobirthing. Again, a very handy tip to have in your personal armoury anytime you feel a bit panicky. An example of a PMR is as follows:
Now you’re calm and focused on your breathing … allow yourself to become aware of all the muscles in your body. Be aware of the feeling at the top of your head … the very top of your head … soothing, calming, relaxing all those tiny muscles in the top of your scalp … feel them releasing, smoothing out, letting go … The feeling carries on now, flowing warmly down your face, those little muscles around your eyes can relax and let go followed by your cheeks and your jaw … notice how it drops open just a little as it releases and let’s go. Let the feeling travel on now … down to your neck, letting go, smoothing out all those muscles … enjoying how deeply relaxed it makes you feel … more deeply relaxed than you have ever felt before … as you let this wonderful feeling flow through you … you may be able to see it … hear it … feel it … gently flowing through you … touching every cell in your body … every nerve, every fibre … from every bone in your body to the very last outer layer of your skin. The feeling travels on now calmly safely and gently into your shoulders … soothing tranquillity floods through them as you release them … as you let them go even more … this wave of relaxation travels on through your left and your right arm … Your hands, your fingers … you may even be aware of a slight tingling sensation in your fingertips as all the remaining tension seeps away. This wonderful, relaxing feeling journeys on now into your chest … your breathing is deeper, slower … focusing on the relaxation your body is experiencing and you instinctively know this is so good for you and good to you … going down into your stomach … soothing, peaceful … releasing and letting go of any tension you’re holding on to there … and it travels on across your hips … smoothing out … relaxing the muscles in your thighs … every nerve … every cell … every fibre of your body filled with this wonderful feeling. Releasing … relaxing your knees … the muscles in your calves … and on down to your feet … until you feel more deeply relaxed than you have ever felt before … you notice this feeling of total deep relaxation has filled every part of you … surrounding you with tranquillity and with peace … it has reached the very last cells on the very tips of your toes … you’re now feeling totally and completely relaxed … more deeply relaxed than you have ever felt before …
Doing a PMR anytime, anywhere (even whilst sitting at your desk) can help you become aware of when you’re holding on to unnecessary tension. Knowing how to let go of that tension is so important for general day to day well-being but it can also be useful when you’re trying to get to sleep. Start at the top of your head and work downwards – exactly how it is written in the above script. And, obviously, for labour it is vitally important because if you’re holding on to any tension in your muscles when the contraction starts, it is going to make it more painful. In addition, being able to totally relax in between contractions is going maximise the benefits of your rest time.
Deepener – guided imagery and visualisation
Depth of trance is not what makes or breaks a hypnosis session and it is very important to stress every person experiences hypnosis in a different way and there is no right or wrong way to do that. The majority of people, however, will find the more they experience the process and the more they come to trust in it, they will experience a deeper level of trance. It can be very helpful to use imagery such as going down in a lift floor by floor, or walking down a series of steps or even using words such as “deeper and deeper” or “down and down” or “more and more”.
It can also help to go to a special place in your mind. I’m aware this seems like I’m advocating very eccentric behaviour, but this is another very useful tool. It can be very calming to imagine yourself somewhere else if you find yourself in a situation you’d rather not be in such as having a blood test for example or having a Caesarean when you had planned for a vaginal birth. It can help you focus your breathing and calm you down which, as we know, is an all-round better feeling to have. This works very well as part of a script but also as a stand-alone relaxation technique. It can be somewhere they have been or it may be somewhere they have only imagined.
An example of a ‘special place’ script is as follows:
Now I’d like you to take yourself to your special place … somewhere you feel safe. It may be somewhere you have actually been … or it may be somewhere you have only ever imagined. Your space may stay the same or it may change … allow your mind to be creative and responsive knowing there is no right or wrong … the most important factor is you feel safe here … calm … relaxed. Pay attention to a particular detail of your special place … maybe it is something you can see. Perhaps it is something you can feel … or maybe it is something you can smell. Really focus in on that detail and notice how it triggers a sense of calm and relaxation in you … maybe even a sense of excitement at what lies ahead. This is your special place … somewhere for you to enjoy as you choose and, from now on, you can return to it at any time it is safe to do so … Negative thoughts cannot reach you here. It’s as if there is a powerful force-field around your special place which means any negative thoughts bounce off and away, leaving you completely unaffected.
This is a pretty generic script and if I was teaching a group class, I would probably use something similar as I wouldn’t necessarily know what each individual would prefer. However, if you’d like to use somewhere specific then you absolutely can. The trick is to make it as ‘real’ as possible. In other the words, the more detail you can give it the more effective it will be. So for example, if your favourite place is the beach, then think about how the sand feels beneath your feet. Is it warm or damp? Do your toes sink in or does it feel powdery? What about the sun – can you feel the warmth on your skin? Is there a breeze? What is the sea doing? Can you hear it? Can you smell it? Maybe your special place is in a cottage by a roaring fire – apply the same principles. Have a go at describing your own special place. You might write down your description in a notebook so that you can easily refer to it in future.
Hypnotic therapeutic suggestions
This is where the real magic of hypnosis comes in and what makes it different from meditation or general relaxation. Every action has a reaction – the role of the post-hypnotic suggestion is to give a better reaction to the situation/feeling/action in the future.
“From now on, every time you place your hand on your shoulder, you feel a sense of calmness drifting over you.”
“And when the time is right for you to go into labour, you handle each contraction with confidence and calm …”
It is worth mentioning that the way suggestions are formed is important. They need to be relevant to the goal you’re aiming to achieve. It is all very well to say you will feel confident in working with the contractions but if you haven’t been given specific ways in which to do that (such as focusing on breathing, ways to increase comfort etc.) the suggestions are not going to be as effective. The sub-conscious is very literal, so you need to use correct time-lines. For example, if you say you’ll “feel more and more calm and confident every day from now until the birth” you might find you’re still feeling anxious at night. A more effective suggestion would be “from now on, with every breath that you take, you feel more and more calm and confident whenever you think about the birth.” Remember – this is only going to work if you want to make the changes. The best suggestions will be positive. The subconscious does not work very well with negatives and doesn’t recognise ‘can’t’ or ‘won’t’. It will respond to “you’ll feel comfortable and calm as you go into labour” but not to “as you go into labour you’ll no longer feel nervous.” Think about what you do want and have a go at writing some post-hypnotic suggestions in your notebook. Reorientation and exit It is very important to bring somebody out of hypnosis gently and carefully, making sure anything they have been told will fade away, such as sounds and awareness, will come back. It can help to give advance warning by counting up and out of hypnosis from 1 to 5:
In a moment I will count from 1 to 5.
On the count of 1 you’ll have full coordination, flexibility and control throughout your entire body … any feelings of heaviness or lightness will return to their true perspective.
On the count of 2 all sounds return to their true perspective …
On the count of 3 you place yourself back in this room being aware of what is around you …
On the count of 4 you come up from this session bringing with you all the benefits …feeling calm, relaxed, re-energised and looking forward to the rest of the day ahead of you.
And on the count of 5 you’ll open your eyes to be wide awake …
So slowly coming up now, beginning to move and stretch on 1, 2, 3, 4, 5.
Eyes open and back to the room.
Further Elements of a Hypnosis Script
There is of course, a lot more that goes into a hypnosis script and if all you want to do is listen to the accompanying downloads that’s absolutely fine.
Feel free to record your own ideas.
Visualisations
One of the most important parts of a hypnosis session is enabling the hypnotysee to visualise what it is they are aiming to achieve. In the case of a hypnobirthing session, giving birth to YOUR baby in the calmest, most confident way possible. However, YOUR brain receives information from all YOUR senses, (our modalities) – sight, hearing, touch, smell and taste (FYI there are actually about 21 senses but we’ll just stick with the usual 5!) It then presents the information internally in a way that allows us to assess it. This informs us whether we need to act on the experience or store it for future reference. We’ll use all of our modalities in any situation, but each of us have a preferred sense that we’re more comfortable using. Obviously, we can all ‘visualise’, as otherwise we would not be able to dream or imagine a route when describing it to another person, but some people will prefer to see that image (visual i.e. sight) others will imagine what it feels like to be there (kinaesthetic i.e. touch) whilst others will prefer to imagine by hearing the sounds around them (auditory i.e. sound). Generic scripts tend to refer to all senses so all of our bases are covered but if you wanted, you could include sensory stimulation specific to you if writing your own.
An earlier visualisation of your special place might have been helpful, but they don’t have to be limited to that particular example. It can be advantageous to visualise what is happening internally during the birthing process – seeing, feeling or experiencing the long muscles of the uterus reaching down to gently pull open the round muscles of the cervix, for example;
- being aware of how it feels as you breathe golden light down to your pelvis, softening and releasing the muscles as you go;
- imagining your baby enjoying the process and how he feels as he is surrounded by your positive energy.
Metaphor is often used within hypnotic visualisations, for example, a slowly opening flower to represent the opening of the cervix or waves to represent the contractions. Metaphors can be very effective within a hypnosis script, but it needs to be relevant. e.g. a boat gently floating on the surface of the sea and easily riding the waves might be more appropriate. This really depends on you and the metaphors you find inspiring and encouraging. You might be very happy with the idea of your vagina opening like a flower, in which case, feel free to use that.
Stick to something which emphasises your strength and endurance, such as travelling a road with lots of hills and slopes and twists and turns along the way.
Future pacing
The mind can be literal and if we have images of ourselves being a certain way or convictions about the way we’ll be responded to, that can become a self-fulfilling prophecy. The more we see ourselves as failing, forgetful, self-conscious etc. the more we tend to live out the reality. The technique of future pacing helps to create new images for the subconscious to portray, so you might imagine, see or feel yourself at some point in the future ‘being’ the person achieving the outcome you want; creating a future where you have had a positive birth experience.
Imagine now it is some time in the future … a time just after your baby has been born. See, feel, hear yourself being amazed and in awe of how incredible the birth experience was … Looking down at your beautiful baby … gazing into your baby’s eyes … feeling the softness of your baby’s skin … inhaling the delicate fragrance of your newborn child. Feel, think about how you stayed relaxed and focused throughout … How you trusted your body … how you relaxed and breathed effectively throughout each contraction. How you went deep within yourself as the contractions became more intense … trusting and accepting the process of birth would take you where you needed to go. How, as the contractions intensified even further, you easily took yourself even deeper into calm and focused breathing. How trusting in your body’s abilities helped to open the birth canal slowly and steadily, allowing your baby to move down and down … breathing effectively to bring rejuvenating oxygen to your muscles … to enable your baby to safely and calmly pass down and down and out of your body and into your waiting arms.
By creating these images, feelings and thoughts, you’re giving yourself a new direction to move towards, giving yourself something ‘real’ and more positive to focus on, creating new ‘memories’ for the sub-conscious to refer to.
When you are in a state of hypnosis when you hear this, your conscious mind is being bypassed and therefore you’re not analysing or criticising each image to see how, why, where or when it should fit into your preconceived idea of how the birth process should be.
In your notebook, write your own future birth story. You can make it as detailed as you want, but remember the focus is on how you feel as you look at your baby, or how she smells or feels in your arms, and how beautifully you focussed on your breathing, as opposed to specific things like having a water birth or getting an epidural.
Triggers
Triggers (also known as anchors) are specific stimuli which influence or create a way of feeling or thinking. They occur naturally all the time – when the doorbell rings, you answer the door; if somebody sneezes, you say ‘bless you’; if somebody were to whisper to you, you’d whisper back. Many of our reactions to certain triggers are because the response has been learnt over time and that behaviour (both good and bad) has become entrenched. In fact, it would be true to say our whole lives consist of triggers of different types that produce different behaviours. Triggers are very powerful when combined with hypnosis and post hypnotic suggestions.
Triggers, such as a touch, a word, taking a deep breath can be created to help bring about positive feelings and responses such as deep relaxation, a feeling of calm and a sense of being in control, very useful when you’re in an environment or situation that, due to its unfamiliarity (anyone thinking birth?) makes you feel anxious or fearful. Again, because the conscious mind is being bypassed, due to the hypnotic state, these suggestions can embed as learnt behaviour without rational thought cancelling it out. Therefore, in the future, as the trigger occurs, the subconscious brings about the positive feelings and responses associated with it. Triggers are even more effective when they reflect your favoured learning modality. If you’re not sure what that is, then include ones that appeal to all your senses to make sure your bases are covered:
Visual Triggers – include suggestions about looking at your partner’s face or a reminder of your soon-to-be-born-baby, such as the scan picture or the outfit you’ll dress them in when they are born. You could even include a suggestion about staring at a mark on the wall.
“Every time you look into your partner’s eyes, you feel more and more relaxed”,
“Every time you focus on the mark on the wall, it encourages you to relax even more deeply”.
Auditory Triggers – sounds such as music, your partner’s voice, humming, repetition of a certain phrase can also act as effective triggers for deep relaxation.
“Every time you hear your partner’s voice/the soothing music you’re reminded to focus on breathing deeply and calmly”.
Suggestions can also be written to counteract any noises that may not be particularly conducive to relaxation:
“Any sounds you hear from inside or outside the room will simply fade into insignificance or help you to relax even more deeply”.
Olfactory Triggers – many people find the smell of aromatherapy oils very relaxing. Burning a particular oil or having a few drops of it on a tissue when you’re practising listening to your hypnosis downloads, acts as a trigger because every time you smell it, the subconscious relates it to a feeling of relaxation.
“Every time you smell the relaxing scent of lavender, you’re soothed and calmed and reminded your body is beautifully, specifically, intricately created to give birth”.
Kinaesthetic Triggers – some labouring women may like to be touched during labour, some may want to be left alone completely, however it is useful to build in some suggestions related to feelings or touch.
“Every time you feel your partner’s touch on your shoulder, your arm, your neck or your back, your muscles respond by relaxing softening and letting go of any remaining tension. Feel your muscles softening … releasing”.
Triggers are especially important in this modern world of ‘managed’ birth, where the majority of babies will be born away from their mothers’ natural habitat, i.e. in hospital. Due to our belief structure and existing Generalised Reality Orientation, the triggers associated with hospitals are likely to do the complete opposite of what we need for birth and create fear and anxiety. Introducing new triggers is a very powerful tool and they can easily be included in a hypnosis script.
Have a think about what triggers you might like to have around you and possibly incorporate into a script and yes, they are very similar to post-hypnotic suggestions. Note down your ideas.
Language
The words we use within the hypnosis scripts are so important because the subconscious is so literal. You want to avoid using words that are negative, create bad feeling and are limited, e.g. Can’t, won’t, must, should, try, don’t etc. and use words that are positive and enabling, e.g. Exciting, calm, serene, powerful, joyful, confident, trusting, powerful etc.
Remember to always focus on what you do want as opposed to what you don’t want. So rather than saying “You don’t feel any fear when thinking about the contractions”, it would be better to say, “the thought of a contraction makes you feel confident and calm”.
Reading speed
Reading a hypnosis script is often the thing people find most difficult because they think they have to sound a certain way or not use any emotion in their voice. It’s actually very simple, just imagine you’re speaking to a young child to try and get them to sleep – you wouldn’t want to get them over excited so your voice would remain calm, you’re not going to speak too loudly because that wouldn’t be relaxing and even though its fine for your voice to show emotion, you wouldn’t want to be too over the top. You also want to make sure you speak slowly so your breathing rhythm naturally slows down. An effective technique to master the correct speed is to repeat the sentence you have just spoken, under your breath. It will seem very odd at first and impossibly slow but the more you practice the more you get used to it. If you’re wanting to ask your partner to record the script for you, have them read this paragraph first.
It can also be really useful to include your name in the recording at certain points, because it makes your subconscious pay attention.
Recognition of the hypnotic state
Depth of trance is not important, nor is fading in an out of what is being said, nor is being able to remember what happened or, indeed remembering every single word. What is important is you’re taking the time out to relax and give your body the opportunity to rest so you can benefit from the relaxation response and start to feel more positive about the prospect of giving birth. If you fall asleep then you’re giving your body what it needs but the likelihood is you’ll wake up when you hear the count up to 5. Remember, everyone is going to experience things differently but some common elements associated with a hypnotic trance are:
- Feelings of weight change – some people will experience feelings of heaviness whilst others feel lighter.
- Some may report feeling they are floating above the surface they are lying/sitting on, whilst others feel as though they are sinking into the floor or their chair.
- Tingling – you may notice a tingly feeling all over your body which is probably due to the dilation of the capillaries, a result of relaxation.
- Time distortion – when someone is in hypnosis, their awareness of time can become quite distorted. Time or the awareness of it is a neocortex manifestation due to our need to measure and assess. In other words, if you’re not using the
analytical part of your mind, time becomes irrelevant and you may find it difficult to accurately work out how long you have been in hypnosis. You can encourage this sense of time distortion during labour with post hypnotic suggestions so your perception is one of having all the time you need to feel wonderfully relaxed and refreshed between each contraction, and the time of each contraction feels as if it is just a few seconds.
-
Heart rate – the heart rate will slow during hypnosis. Internalised emotional response – you may experience intense emotional feelings that someone observing you might not even be able to notice. This could be anywhere on the scale between excessive happiness or dramatic tears and it could be physical such as an increased heart rate or emotional.
This list is not exhaustive.
A good indicator you’ve been hypnotised is when you’re re-orientated, you may take a little while to return completely to awareness, you may even feel a little dazed. It’s always a good idea to give yourself a bit of time when you first come out of the trance before you spring up and carry on with the rest of your day.
Abreactions
An abreaction is an emotional release. It can happen because you may have let go of an intense fear or even because you have had some sort of internal revelation and it can be quite extreme. It may happen during the session or can happen once you have been re-orientated. It may be quite alarming to experience, but it is actually very positive and shows the hypnosis has had a profound effect. If it does happen, use your exhalation breath to calm yourself down and give yourself a minute or two just to ground yourself.
Use the relaxation techniques that you feel will help to ground you.
Self-hypnosis
The purpose of teaching you hypnosis techniques for use in childbirth is really equipping you with the ability to hypnotise yourself. All of the relaxation techniques we’ve talked about are all methods by which you can take yourself into a hypnotic state.
Affirmations
We’re constantly giving ourselves messages, in line with our internal beliefs, that are associated with the belief we have in ourselves. This part of our belief system is built up by other people based on their belief systems which is based on the belief system of another set of people, and so on. In these cases, we cannot often get a reliable external source we can test things against, so when the details are suggested over and over again, they form our belief system and become our point of reference. Any time something different is suggested, our conscious brain steps in and rejects it because it does not correspond with what our subconscious is saying.
Every time we have a thought there is a hormonal response in our bodies, known as an ideomotor response, which then creates a physical effect. For example, a certain thought may cause you to develop goose-bumps or, someone only has to mention head-lice and you’ll probably find your head starts itching, or when watching a scary movie, even though the frightening aspects are suggested and you know it’s not real, you physically respond as though it is. You can see, therefore, why it would be helpful to use positive thoughts to help change your mind-set. Yes, I am aware this is more easily said than done but there is a handy little tool known as affirmations, basically positive thoughts, that can make a huge difference. The human animal, runs on a series of patterns based on our beliefs and the beliefs of others and learnt behaviours. It can be very difficult to change these behaviours and beliefs just by telling ourselves to do it (imagine what a different world we would live in if that was the case!). Affirmations help to stop those patterns running and give you a choice of how you want to feel. They can also help by stopping the pattern of anxiety from running. When we feel anxious, we ruminate over and over again on the things that make us anxious creating a hamster wheel effect which goes round and round continuously inside our brains. Using affirmations is similar to putting a stick between the spokes of the wheel and stopping it – giving you the choice to get off. Affirmations, compound the positive suggestions being given under hypnosis as well as producing a positive ideomotor response and therefore a positive physical effect. Affirmations are a useful tool to use if you catch yourself thinking negatively about your ability to give birth or if you’re told a distressing birth story. It can be quite tricky to get the concept of wording affirmations in a way that doesn’t sound as though you’re just throwing words around for the sake of it. But, just as when writing a hypnosis script, think about what you do want as opposed to what you don’t want. “I don’t want an epidural” for example, may sound positive as you may have decided to give birth without the use of drugs, but your subconscious mind will be hearing “I do want an epidural” because it doesn’t respond to negatives (think about what happens when you’re told not to think of pink elephants!!) A more effective affirmation would be “I trust in my body’s ability to work with my contractions”.
In a way, affirmations are about re-framing the things we’re worried about and by doing so they become less scary.
Try it now.
Write down three things that make you anxious about birth and then re-frame them into an affirmation.
For example, instead of: “I’m worried about labour taking a long time” Reframe/Affirmation: “I have all the endurance, strength and stamina I need to birth my baby”
If you’re finding it hard to write your own, there are plenty of birth affirmations on the internet but some you may like are:
Giving birth is a normal and natural occurrence
My body is designed to have a peaceful, calm and joyous birth I
I’m more and more calm and relaxed when I think about the birth
I know my baby feels my calmness and confidence
I trust in my ability to give birth
My body knows exactly what it is doing
I’m confident in my ability to give birth
I’m excited at the amazing journey ahead of me
Check out the “Goody Bag” for your The Ripple Effect Affirmation cards.


Another exercise you can try is to have a read through these and make a note of the ones you like but also the ones you’d like to say but maybe can’t quite bring yourself to believe at this point.
The ones you find difficult are the ones you need to challenge yourself to say. The mind and body work as one, remember, so if you’re giving yourself a positive thought, you’re creating an ideomotor response. You don’t need to believe it, thinking it is enough – remember the head lice?!
Affirmations work in the same way as post-hypnotic suggestions – the more you read/say them the more the subconscious accepts them as reality.
What you may want to do is to choose the ones that resonate with you and stick them up so your eye can skim over them every time you see them.
Or write them on post it notes and stick them around the room or inside cupboard doors. If you’re a creative person, you could print out some of your favourite photographs and attach the affirmations to those or draw beautiful pictures to accompany them.
Some clients create vision boards of affirmations and taken them with to the birth.
You could also record them or get your partner to record them so you’re listening to them, just like you would the hypnosis downloads. Use your name, to make the subconscious sit up and listen and make them current – i.e. write about what is happening as opposed to what will happen so “I remain calm and relaxed throughout each contraction” instead of “I will remain calm and relaxed throughout each contraction”.
Your mind is strong, stronger than you may have previously given it credit for. Using tools such as affirmations can have a powerfully, positive effect on how you feel. They can be used in combination with hypnosis or on their own, either way they are an extremely effective way of changing your mindset and helping you to look forward to the prospect of giving birth.
Mammalising Birth
Allowing ‘our monkey’ to do it
A mammal is a classification of animal in which the female of the species grows her baby within her body, gives birth to it and feeds if from her own milk supply. Typically, a mammal left to give birth instinctively will:
- Usually give birth in the dark, once she has found somewhere safe to do it.
- Moan quietly and rhythmically, but appear relaxed and calm at the same time.
We know animals can exhibit signs of pain and fear if they are trapped or injured but they do not appear to show any of those signs whilst giving birth, they simply allow their bodies to get on with it, just as they do with any other physiological function. The reason? No one has taught them they need to be frightened of birth. Some species are protected by other members of their group (dolphins and elephants), and some prefer to be on their own (cats). Interestingly, when humans have tried to observe the process (as in research trials on chimpanzees) the animals delay giving birth until the humans have gone away (Newton, 1971.) This makes total sense when you think about the affect the ‘fight or flight’ response has on birth – it stops the labour so the mother can get to a place of safety. Animals rely on their instincts to know when a place is safe or when there is danger about. Human females, being mammals, would, ideally give birth in the same way. We share the same physiological processes and functions for breathing, heart pumping, digesting food and expelling waste, reproduction and nurturing of our young. The Limbic and Reptilian parts of our brains are exactly the same as our four-legged counterparts, however as humans have developed a higher level of intelligence and become upright to walk on two legs instead of four, we’ve developed the Neocortex or new brain.
The Neocortex is excellent for analysing, criticizing and decision making but it is no good for giving birth, because it takes us out of the state needed for our bodies to do what is necessary. Ina May Gaskin, in her book Ina May’s Guide to Childbirth (2003) recommends letting your monkey do it when it comes to birth which means do not let the over-busy mind interfere with the ancient wisdom of the body.
She goes on to list things monkeys don’t do in labour, that many women do that interferes with labour:
- Monkeys don’t think of technology as necessary to birth-giving.
- Monkeys don’t obsess about their bodies being inadequate.
- Monkeys don’t blame their condition on anybody else.
- Monkeys don’t do Math[sic] about their dilation to speculate how long labour will take.
- Monkeys in labour get into the position that feels best, not the one they’re told to assume.
- Monkeys aren’t self-conscious about making noise, farting, or pooping during labour. All Queens, duchesses and movie stars poop – every day, if they’re healthy. The problems happen when women feel acting in that way is somehow shameful, disgusting and embarrassing.
Sphincter law
Sphincter muscles are circular muscles designed to keep something in until it is time to release it. We’ve lots of sphincter muscles within our bodies, but the most commonly known ones are in our bladder and anus. Ina May discovered the same rules that apply to a human’s ability to release those sphincter muscles also apply to the sphincter muscle of the cervix. This she named Sphincter Law, the principles of which are as follows:
- Excretory, cervical and vaginal sphincters function best in an atmosphere of intimacy and privacy – for example, a bathroom with a locking door or a bedroom, where interruption is unlikely or impossible
- These sphincters cannot be opened at will and do not respond well to commands (such as “Push!” or “Relax!”).
- When a person’s sphincter is in the process of opening, it may suddenly close down if that person becomes upset, frightened, humiliated or self-conscious. Why? High levels of Adrenalin in the bloodstream do not favour (sometimes they actually prevent) the opening of the sphincters.
- The state of relaxation of the mouth and jaw is directly correlated to the ability of the cervix, the vagina and the anus to open to full capacity. (Gaskin, 2003) The importance of the birth environment and building a nest
All of the above, ties in so beautifully with all we’ve learnt about hypnobirthing and how it works, but knowing it and putting it into action are two very different things.
One technique that can make a massive difference is thinking about your chosen birth environment and how it can be adapted to support all you have now learnt. As we now know, information from the world around us, controls us more than we’re consciously aware of, because it feeds in to and off of our internal belief system. So, stimuli from the outside world can trigger fear and terror and fight or flight reactions.
To most people, despite the conscious decision to give birth in hospital because that is where they think they will feel safest, the subconscious messages they will be receiving, are ones that associate hospitals with sickness, disease and in some cases death because that ties in to what they have subconsciously learnt when growing up.
On top of which, humans are the only species of mammal that moves away from the safe, familiar surroundings of home when giving birth, to go somewhere their subconscious sees as threatening. No wonder many women’s contractions stop when they get to hospital, it is due to the Adrenalin released in response to the danger signals received by their subconscious.
However, the environment can also send signals that all is calm and safe and then the response is comfort and relaxation and calm. This is enhanced if the sensory information comes via the skin or nose as these processes, to a large extent, take place unconsciously. All mammals rely on these senses to give birth safely. The reality is most women will decide to give birth in hospital, because that is what society has come to believe is best but it can be difficult to ‘let your monkey do it’ surrounded by the interventions, interruptions and time constraints often surrounding a hospital birth. But the good news is that the negative stimuli can be reduced and replaced with things you associate with calm and relaxation. Think back to the Triggers section – how they can be accepted as learnt behaviour through post-hypnotic suggestion. Really think about the smells and the sensations and the sounds and the sights you want to have around you during labour and birth and start making them part of your hypnosis sessions . The sooner these can become a familiar part of the self-hypnosis/hypnosis process, the more effective they will be when you go into labour. This is particularly important if you’re having a more medical birth for whatever reason.
Think about how you’ll set up your nest at home for the early stages of labour and which items will you easily be able to transfer to a hospital environment? The importance of the environment is not to be underestimated.
Studies have shown the birth environment may aggravate a labouring woman’s anxiety and pain levels.
- Loud noises increase fear, which we know can make someone more sensitive to pain.
- The perception of pain can also be influenced by the brightness of the room, the temperature and the feeling of being observed because of the stress hormones that are stimulated in these situations.
It is, therefore, essential the stress-inducing components are reduced as much as possible. Even if you have decided an epidural is an absolute must for you – once it has been sited turn the lights off in the room, put some relaxing music on and let the Oxytocin flow!
ENVIRONMENT
What are some of the things you may want to consider using to support the process of birth?
Essential Oils – When listening to your downloads in the lead up, make sure you can smell your chosen oil. Your subconscious will then associate that particular smell with relaxation and safety
Your pillows – so much nicer to bury your head in, in between contractions. They all also smell of you and feel familiar which subconsciously equals safety Your blanket – Great to hide under during a contraction if you’re feeling observed. It also makes a hospital environment look less ‘hospitaly’ because it looks familiar to you
Wear you own clothes – You’re not ill, you’re not a patient, you don’t need to wear a hospital gown
Turn the Lights out – Every room in the hospital, birth centre or delivery suite has a light switch.
Turn it off! Bright lights make you feel observed, darkness makes you feel private. In addition, when it is dark, our eyes see it is dark which sends a message to the brain to produce melatonin – our sleepy hormone. Sleepy hormones make us feel chilled and relaxed and boosts Oxytocin. Win Win!
Fairy lights – I love a fairy light! You can wrap a string of them around the back of the chair and it transforms into something magical. Bring them with you to the hospital or LED candles (no real ones due to all the oxygen floating about!!!). Immediately the room becomes much more romantic and it feels like your space.
Lovely things to eat – tempting morsels of food are not only essential to keep your energy levels up but they can be used to reward you after each contraction.
Headphones – Hospitals are noisy places and you may not want to hear general chatter or other women giving birth so block out the sound by listening to your own music. Headphones also help you to feel as though you’re in your own little private world – again reducing the feelings of observation.
It is worth noting, If a woman’s labour stalled whilst in the care of someone like Ina May Gaskin, she would be asked what is bothering her and she would be given the chance of expressing any concerns, the environment would be made more conducive and she would be given time to feel more comfortable both emotionally and physically.
If a woman’s labour stalled in a hospital, more often than not, artificial hormones would be used to help get the contractions going again.
Making love
The hormones involved in making love, namely Oxytocin and Endorphins, are the same hormones involved in giving birth. Watch the “Conception” video and this highlights the pressure birthing couples are under to perform.
Imagine, making love in a brightly lit room, surrounded by people telling you what positions to be in and keeping notes of your progress? Most people would find that extremely difficult and yet, that is the environment in which women are expected to give birth. Just as most people prefer intimacy and privacy and the ability to move how they want when making love, so too would they prefer it when giving birth. It’s our natural mammalistic instinct. Whilst birth can and does happen in environments which may not be classed as ‘romantic’ if your labour is slowing down, if you’re anxious or scared if you’re wanting to avoid intervention, making these changes can make a huge difference.
Induction
One of the most common interventions pregnant women face is induction i.e. artificially initiated labour. The World Health Organisation (WHO) states 25% of all ‘deliveries’ at term are induced (2011). The healthcare trust a woman is under, will determine when she will be ‘offered’ induction (although many women are made to feel as though there is no choice.) The topic of induction is huge and if I went into everything here, I could have a whole book as opposed to a mention in a chapter.
Luckily, Sara Wickham has written “Inducing labour – making informed decisions” which is certainly worth a read, as it is something commonplace within our birthing culture. Induction of labour (IOL) for being ‘overdue’ is one of the most common reasons for induction that you’re likely to be faced with. The actual due date is very difficult to determine, as is the individual’s natural gestation period.
There is no actual evidence to support the belief that Naegele’s rule (the little wheel midwives use to calculate due date, based on the first day of your last menstrual period) is accurate.
Nor is there robust evidence to say being induced before 42 weeks is unequivocally safer for the baby (Wickham, 2018).
However, a lot of these practices have been happening for so long, they’ve become entrenched. This is known as practice-based preaching as opposed to evidence-based teaching.
The issue with induction when it is on a ‘just in case’ basis is if the body and baby are not ready to go into labour, it to go into labour, it can lead to a long drawn out process, considerably more uncomfortable than when a woman goes into spontaneous labour. There is also a massively increased chance that IOL can lead to instrumental birth, tearing, episiotomy and/or caesarean because of the cascade of intervention. One study found induction increases the chance of Caesarean by 20% for first time mothers (Reed, R., 2016.) It has become common practice for women to be offered a stretch and sweep from about 37 weeks, when midwife or doctor during a vaginal examination, sweep a finger around or within the opening of the cervix, in an attempt to stimulate the body’s natural Prostaglandin production. REMEMBER – YOU MUST GIVE CONSENT … if they do an internal examination and as they come out they say “ohh I just did a quick sweep whilst I was in there” … that’s ASSAULT and you should definitely ask for the senior midwife on duty and ask for a change of midwife … THEY MUST SEEK YOUR CONSENT BEFORE DOING A SWEEP …
However, research has shown a sweep does not seem to produce “clinically important benefits” (Boulvain et al 2005:2). It comes down to personal choice whether to have one or not, but I usually remind my clients to advise their care givers that if the cervix is not easily found (remember it points backwards during pregnancy and only starts to come forward when the time is right) they should refrain from looking for it! If the mother agrees to an induction the first stage (depending on what is happening with the cervix already) is synthetic Prostaglandin, generally in the form of a pessary, tablet or gel which is placed high in the vagina during a vaginal examination. Some hospitals use a version of Prostaglandin, known as Propess, which looks like a very small tampon and has a similar string to pull it out if and when it needs to be removed. Prostaglandins can sometimes cause strong contractions very quickly which the baby (and the mum!) could find very stressful so there is usually a period of electronic foetal monitoring for 30-60 minutes after insertion to check that baby’s heartbeat remains within normal limits. Depending on whether a woman has had a baby before, or how ready or not her body is to go into labour, affects how many doses of Prostaglandin she may require. Sometimes women are permitted to go home in between insertion and re-examination, other times they are asked to stay in hospital. As with any form of intervention, there are risks such as uterine hyperstimulation (extremely strong and frequent contractions), foetal distress, increase in maternal temperature, infection etc.
Some hospitals will use a device called a Cooks Balloon which is inserted through the neck of the cervix and then inflated. The idea is it puts pressure on the cervix to encourage dilation. There is less risk of uterine hyperstimulation with this method, but it can be fairly uncomfortable and a small
You Can Still Use Hypnobirthing
Augmentation
Augmentation means speeding labour up once it has started. The methods used are very similar to induction, in that it could involve either or both ARM and Syntocinon. As with everything that could interrupt the physiological production of hormones, parents would be wise to establish whether augmentation was being suggested because of an emergency and if not, what would be the benefits and risks of the suggested procedures.
Forceps and ventouse
Both are instruments used in an assisted birth which may have become necessary either because the baby is showing signs of foetal distress and needs to be born quickly, baby is in an awkward position or mum is just too exhausted and does not have enough energy to push her baby out.
Forceps look like large salad servers that come in two parts. The mother many need an episiotomy (cut) in the perineum for the curved bit (unfortunately called a ‘blade’!) to be placed in the vagina and fitted around the baby’s head. Once the second ‘blade’ has been inserted, the handles clip together to hold the baby’s head firmly (but cannot be squeezed any tighter). The obstetrician will then pull as the mother pushes during a contraction.
A ventouse (often known as a Kiwi Cup) works in a similar fashion in that it is applied to the baby’s head whilst it is still in the vagina. Suction is created by pumping the handle and then the obstetrician pulls while the mother pushes. The decision between whether forceps or ventouse is used depends very much on the preference of the care giver and the situation it is being used for.
Compared to forceps – ventouse is:
- Less likely to be successful at helping the baby to be born
- More likely to leave your baby with a temporary swelling on her head (cephalohematoma)
- Less likely to cause significant damage to the perineum or vagina
Compared to ventouse – forceps are:
- More likely to be successful at helping the baby to be born
- More likely to cause redness or slight bruising on the side of the baby’s face
- More likely to involve an episiotomy, a severe tear, or both
- More likely to cause significant damage to the perineum and vagina
- Cause short-term incontinence problems, such as being unable to control the bladder, wind or bowel movements It may appear the ventouse is the best option, as it causes less trauma to mum and baby, but they can’t be used for babies born before the 34th week of pregnancy (as the baby’s skull is too soft to cope with the pressure of the vacuum) or if the baby is lying face first.
- If the baby needs to be born quickly, forceps are often the better choice as they are more likely to be successful and trying one instrument first and then moving on to another may cause more damage.
They sound absolutely gruesome and I have to admit, they are not my favourite way of helping a baby into this world,
However, if it comes to needing either of them, they can save lives. The best way to avoid needing them (or massively reducing the chances of needing them) is to stay at home as long as possible, remain as upright as possible during labour, avoid intervention and epidural as long as it is safe to do so, listen to your body during the pushing stage and refrain from lying on your back.
Episiotomy
Episiotomies used to be done routinely but now are only given if the midwife feels the the perineum will tear badly. However, this is also, unfortunately, a practice that is based on little (and questionable) evidence which also claimed that an episiotomy prevented brain damage to the baby because it meant it no longer had to pound his head against the perineum (Oxorn-Foote H, 1986)!
There is also the belief that a smooth cut through the muscle will heal better than a jagged tear. In fact, the opposite is true – it is much easier for a tear to heal because the jagged edges join together more easily than the smooth edges of a cut.
An episiotomy will be given (usually after a local anaesthetic has been administered) if forceps become necessary or if the baby needs more room to be born but they will not prevent more serious tears from occurring (Sleep, Roberts and Chalmers, 1989)
Tears
Although tears are not an intervention as such, it seems appropriate to mention them at the same time as we’re talking about episiotomies.
There are 4 types ranging from mild to severe:
First-degree vaginal tear
This is the least severe and involves only the skin around the vaginal opening. They are not particularly painful and will usually heal on their own without the need for any stitches.
Second-degree vaginal tear
Second-degree tears involve both the vaginal tissue and the perineal muscles. They do require stitches but will usually heal within a few weeks.
Third-degree vaginal tear
Third-degree tears involve the vaginal tissues, the perineal muscles and the anal sphincter which are the muscles that surround the anus. These tears will require an obstetrician to repair the damage and will be done in an operating theatre as opposed to the delivery room. It could also take several months to heal. Complications such as faecal incontinence and painful intercourse are possible.
Fourth-degree vaginal tear
Fourth degree tears are the most severe. They involve the vaginal tissues, the perineal muscles, anal sphincter and the tissue lining the rectum. Again, these need repairing in an operating theatre, can take many months to heal and complications mentioned above are possible.
After your baby has been born the midwife will check your perineum to see whether it is intact or not and whether any repairs are going to be needed.
Warning: it may (actually it should) involve a finger up the anus to check there is no tear in the back passage. Any injury in that part of the body is going to involve some discomfort whilst it heals.
Obviously the most severe tears are going to take a lot longer and may require physio as well as treatment by someone who specialises in the field. Any of the tears above are susceptible to infection so it’s important you’re scrupulous with your personal hygiene, especially as there will still be blood loss from the pregnancy (lochia). It is important to wear specific maternity pads because the ones we buy for periods are often plastic backed and can make the area sweat more. You’ll be encouraged to change maternity pads regularly to prevent infection and not to use anything too perfumed for obvious reasons.
If you find it stings when you do a wee, it can help to pour warm water over the area as you pee to dilute it – weeing in the shower or in the bath can also help and is probably an easier manoeuvre!
Doing the first poo, after stitches can be interesting because it may feel as though everything is going to fall out – it won’t, but it is unnerving nevertheless.
Holding a wadded-up piece of toilet paper against the perineum can give peace of mind. It can also help to make sure you drink lots and have lots of fibre in your diet to keep stools soft.
There is some evidence to suggest the perineal massage can help avoid tears (Beckmann and Garrett, 2006) and anecdotally, there seems to be lots of evidence to support that. Perineal massage helps because it enables you to make both physical and mental contact with your vagina. I know that sounds weird but, certainly in Western culture, we don’t tend to talk about ‘down there’ unless you are in a Ripple class when we talk about EVERYTHING and even though we know where a baby comes out of, it often makes us feel squeamish even in the context of childbirth. Spending a bit of time prior to birth, exploring, stretching the muscles around the vagina helps to make everything, including accepting that’s where a baby’s head is going to emerge from, a lot more normal.
Caesarean birth
A Caesarean birth is usually performed when a vaginal birth could put mum or unborn baby at risk. This is a huge topic and there are whole books written about the subject. The World Health Organisation says the Caesarean rate should be 10-15% in order to make a difference and save lives. The national average in the UK is nearly 30%, with some hospitals having an even higher rate.
Ina May Gaskin has a Caesarean rate of 1.4%. This suggests that some Caesareans are happening when they could have been avoided, perhaps as the end of a cascade of intervention.
There are three types of Caesareans:
Planned or elective
The operation is scheduled before the mother goes into labour.
This can be because of maternal choice, multiple birth, position of the baby (i.e. breech – bottom or feet first or transverse – lying across) which makes it difficult for the baby to fit through the pelvis, maternal infection such as genital herpes or placenta praevia (blocking the exit of the womb).
Unplanned or emergency
The decision to perform a Caesarean happens once labour has started, most commonly done because of foetal distress or lack of labour progression.
Despite the name, it is NOT an actual emergency although it can be very frightening if you hear that word.
Crash or category 1
This is when the situation is life threatening and baby needs to be born immediately (this is the real emergency).
This will be done under general anaesthetic and partners will not be allowed into the room.
The way birth is presented many women feel having a Caesarean is easier than giving birth vaginally. They feel it takes away any uncertainty about when the baby will be born and for many, it is the less frightening option with the bonus that no damage needs to happen anywhere near the vagina.
The fact of the matter is, physiological birth is not meant to be frightening or damaging. If conducted in the way we’ve previously discussed, the chances of real problems occurring are low and much more likely to happen if the birth is interfered with. Recovery from a physiological birth is almost instantaneous, with the pain forgotten as soon as they see their baby.
A Caesarean takes a good 6 weeks to recover from and it is major abdominal surgery. Being born this way can cause breathing difficulties in the baby because it hasn’t been through the intense contractions that happen at the end of labour which help squeeze fluid out of his lungs and prepare them for life on the outside (although most if these issues are slightly more of a concern with an elective caesarean because labour may not have officially started before the baby was born)
However, perhaps most importantly, a Caesarean birth is much ‘cleaner’ than vaginal birth.
In other words, the baby does not come into contact with any of the good bacteria in the vagina nor has contact with poo on his way out. All of which, contribute to the very important job of seeding the microbiome i.e. preparing the baby’s very sterile immune system for contact with a very un-sterile world. There is a lot of research on this currently going on.
A baby born by Caesarean misses out on all of that. There is still a load of research to be done, but there is some evidence to suggest babies born by caesarean who miss out on these important elements are going to have a higher chance of contracting illnesses and health conditions (Dietert R. and Dietert J., 2012).
In addition, future fertility can be affected and breastfeeding and bonding may be delayed because those all-important, hormones won’t be produced in the quantities needed due to the birth process being ‘interrupted’.
There may be lack of skin to skin contact or, because of being in theatre, and/or, depending on the circumstances necessitating the procedure, there may be separation of mother and baby for an extended period of time.
The mother and baby are likely to have high levels of stress hormones during and immediately after birth, because there has not been the huge surge of Oxytocin at birth which calms everybody down.
Please be aware the these risks are rare but it is important to know all the information when making your decisions.
That is not to say if you were to give birth by Caesarean, you can forget ever having a relationship with your child or there’s no way you’ll be able to breast feed. It is important for you to know even if you’re initially separated from your baby, as soon as you’re reunited, you can spend as much time as you need skin to skin with your baby to give the hormones a fighting chance (this applies however your baby has been born). Providing baby is OK there is no reason why you can’t have immediate skin to skin in theatre. All you need to do is either wear your gown back to front, so the open bit is at the front, or wear it evening gown style, as in off one shoulder. These small changes in how operating gowns can be worn, make skin to skin so much easier.
Any claims baby will be cold in theatre if not wrapped up in a towel … rubbish … skin to skin regulates body temperature!
You can also ask to have catheters sited in your non-dominant hand and to ensure all heart monitor pads etc. are attached to your back and any leads to be passed under the table. You can also ask for the screen to be lowered slightly at the point of birth, so you can see your baby being born (Don’t worry, you won’t be able to see any of the gory bits because your tummy will be in the way!)
Caesarean birth can be where your birth ends up, it can become a necessity or it can be a deliberate choice – it is still the birth of your baby and you can still use hypnobirthing!! All the principles about remaining calm are just as relevant and a lot of the affirmations can be adapted to suit an abdominal birth. If you know well in advance that you’re having a caesarean let your hypnobirthing practitioner know. You could also do some research on Gentle Caesareans, as pioneered by Professor Phillip Bennet, Consultant Obstetrician to Imperial Healthcare NHS Trust at Queen Charlottes and Hammersmith Hospitals. I have already mentioned several factors but the aim is basically to replicate a vaginal birth and the pressure on the baby’s lungs as much as possible by facilitating the baby to slowly push/manouver itself through the abdominal incision.
It used to be thought that once you had a caesarean you would need to have a caesarean for any future births because of the chance of scar rupture. Whilst that is certainly an option, there are also such things as a VBAC (Vaginal Birth After Caesarean) which you’re more likely to achieve by following all the suggestions in the first few parts of this book. The recent NICE (National Institute for Clinical Excellence) guidelines (2019) recommends continuous monitoring is not needed, nor is having a cannula and you can use water – so, good news all round! Monitoring The whole reason we have midwives with us when we give birth is so they can check we’re alright, no sudden fevers or loss of blood pressure, and our babies are coping well with the process of labour. We’re monitored with blood pressure cuffs and thermometers and our babies heartbeats are monitored. For the majority of women, intermittent monitoring i.e. listening in every so often with a hand-held Doppler or Pinard Stethoscope is sufficient. By doing this, the midwife is able to build up a picture of how the baby’s heartbeat is coping with the contractions. By listening in every 15 minutes or so in the earlier stages and then after every contraction in the later stages, she can tell which babies are coping fine and which may need a little more help.
Some pregnancies are deemed too high a risk to rely on intermittent monitoring alone and ‘require’ Electronic Foetal Monitoring (EFM) instead. This requires two transducers to be attached to the mother’s stomach – one reads the intensity of her contractions and the other monitors the baby’s heart. These transducers are connected by wires to a monitor (in some hospitals they have waterproof wireless telemetry monitors) which then print out a cardiotocograph to be analysed. Whether a midwife is listening in, or reading the results from the printout, they are looking for any changes that are out of the ordinary. The problem with EFM is it’s not as accurate as you might expect. They have become very popular amongst the medical profession because in the over worked, minimal staff, environment of a lot of modern NHS hospitals, it is a lot easier to have several women hooked up to machines and be able to flit between them reading printouts, than it is to ensure babies are listened to on a regular basis. Also, as hospitals and maternity practices have become more and more risk adverse, it helps to have ‘evidence’ of reasons why procedures were performed in case something were to go wrong. The issue is EFM’s are notoriously inaccurate with a false positive rate exceeding 99% (Sartwelle and Johnston 2014). Bewley and Brailton (2018) in their article for the BMJ state:
“Cochrane, The International Federation of Gynaecology & Obstetrics, and the National Institute of Health and Care Excellence have all said no evidence shows human or computerised interpretation of cardiotocographs reduce the rates of intrapartum stillbirth and cerebral palsy, but it can cause maternal harm.” In other words, invasive procedures being performed on mothers and babies are not always necessary because if there is written ‘evidence’ on a cardiotocograph and the hospital were seen not to have acted on it, they would be liable if something did go wrong. In addition, they ‘require’ the mother to be lying on her back to get an accurate reading which leads to more painful contractions, which can lead to epidural requests, which can slow labour down, which requires syntocinon, which can lead to foetal distress and so on and so on. By the way – you really DON’T have to lie down if you’re being monitored. It is definitely easier for you to be doing so, as far as the caregivers are concerned as the transducers are less likely to come off. However, you’re giving birth so you don’t need to be obliging. If it is easier for you to stand up – stand up! If the monitor comes off, someone else can hold it in place.
Vaginal exams
Vaginal examinations (VE’s) have become a ‘normal’ part of intrapartum care. Whilst an examination can give the mother, who has been labouring for hours, the good news she’s been waiting for i.e. Her cervix has now reached 4 cm, so she is ‘officially’ in labour, it can be equally as demoralising if she is given a figure which is not as high as she had hoped. It disregards the mother’s instinctive knowledge by reinforcing the belief she knows less than the experts. They are invasive – some women find them uncomfortable, and some, especially those who are survivors of sexual abuse, can find them very traumatic. They can introduce infection; they can cause amniotic sacs to break accidentally and one practitioner can measure cervical dilation completely differently from another. In addition, they don’t really give an awful lot of information and should be interpreted in context to everything else going on. So, are they necessary? In some circumstances it can be a good idea to perform a VE, but it’s use to determine labour progress is questionable (Reed, 2015). Admittedly, midwives have been performing these examinations for centuries, however they were usually carried out in response to a suspected pathology (something wrong) such as an obstructed labour or a mal-presentation, rather than being routine. In other words, a VE provided an assessment of a complication and helped carers determine what to do about it (Reed, 2015). As we know, modern maternity practices are based on the development of medicine, which was heavily influenced by the industrial revolution, amongst other things, and, there was an understanding that the body, like a machine, could be broken down into specific parts that could be studied separately. So, a birthing woman was divided into ‘uterus’, ‘cervix’ and ‘baby’ and this very simplified but wholly incorrect representation has underpinned birth education, its progress and the necessary practices that should accompany it, ever since. The partogram, the graph on which dilation and progress is plotted, became established practice in the 70’s and, in order for midwives to plot the graph, they needed to do regular VE’s.
However, as previously discussed, actual labour patterns do not fit the timeframes prescribed by partograms and, there is no evidence to suggest routine VE’s in labour improve outcomes for either the mother or her baby. A Cochrane Review (2013), as cited in Rachel Reed’s article, states “We identified no convincing evidence to support, or reject, the use of routine vaginal examinations in labour …” Sounds promising, right? Well, yes it does, but the same review also states: “Given the fact the partogram is currently in widespread use and generally accepted, it appears reasonable, until stronger evidence is available, that partogram use should be locally determined.” A common situation, when it comes to maternity – interventions implemented without robust evidence require ‘stronger’ evidence before they are removed or changed. Unfortunately, it is unlikely that this strong evidence (i.e. randomised controlled trials) will be gained due to research ethics and the culture of maternity systems (Reed, 2015). Nevertheless, women should be informed it is entirely their choice as to whether they want a VE and it is their right to consent or decline it. Hospital policy is to offer to do a VE, if the midwives have done that, they are using correct practice. If a mother declines and the midwife or doctor does it anyway, then it is classed as assault. A woman always has the right to say I DO NOT CONSENT!!
In reality it can be difficult for a birthing person to say on arrival in triage or in the labour ward/birth centre, that she doesn’t want any VE’s. This isn’t always the case but those that have chosen to decline a VE may be on the receiving end of being refused entry to the labour ward or birth centre or pain management is denied. Maternity staff don’t always handle their response to your choices positively.
Pain Relief
To recap; the body is perfectly capable of managing labour with its own hormones, breathing, relaxation, safe dark environment, eating, drinking and resting to keep the energy up, all enable the body to work to the best of its abilities. However, some women are going to be particularly anxious about birth, some will feel safer knowing they have the drugs on board, sometimes the circumstances of the birth means more medical forms of pain relief become necessary, even if they were not what was originally wanted. Every form of pain relief has its place and there is no right or wrong way of giving birth but medical forms of pain relief are a form of intervention and some of them can interfere with the production of hormones making further intervention more likely. Also, bear in mind that some options for pain relief are not going to be available until you get to hospital and that can sometimes take a while. Hypnobirthing can help you to remain calm until you can get to hospital and gain access to your drug of choice. By the way, I’m going to be using the word ‘pain’ – you already know my feelings on that!
T.E.N.S
T.E.N.S stands for Transcutaneous Electrical Nerve Stimulation. It is a small machine which generates pulses of electrical energy through 4 sticky pads (electrodes) attached to your back.
The electrical pulses are felt as tingly sensations which encourage your body to produce Endorphins. These travel to the brain faster than the feelings of discomfort caused by the contractions. Every time you experience a contraction, you press the boost button attached to the machine and by the time the ‘pain’ signals reach the brain they are distorted and lessened by the Endorphins already there. T.E.N.S machines can be hired or bought, and they work best if they are put on as soon as you’re aware you’re experiencing contractions.
WARNING TO PARTNERS:
if your partner has been using her T.E.N.S machine throughout labour, the chances are, by the time the baby has been born, it will have been turned up very high.
DO NOT touch the underside of the pads until the machine has been turned off.
Her Endorphin levels will be sky high, yours won’t and those tiny little gadgets pack quite a punch.
I have been on the receiving end of these beauties … it certainly didn’t fling me from one side of the room to the other but I did have an interesting conversation with the dad who was adamant he had switched it off but had actually hit the BURST button!!! Hmm. the air was a little blue … to say the least … when I tried to remove it.
We did have a good chuckle about it when we were reflecting. Especially as we were removing them in a bathroom that was lit by candles!
Liked Because:
No risks to mum or baby Non-invasive
Mum remains in control
Can be used from very 1st contraction whether mum is at home or in hospital
Disliked Because:
Can take a bit of time to work effectively (hence the need to put it on early)
Cannot be used in water
Some women may find the pain-relief inadequate
Water
Water is an extremely effective pain-management tool. Being submerged in warm water at the most intense part of labour, can be just as effective for some women as an epidural is for others.
Using a bath or the shower in the early stages can also be helpful, especially if you need to rest because the early/excitement phase has been long and you haven’t really slept. The movement or flow of warm water on the skin also encourages your body to produce Endorphins – the body’s natural pain killers. It stands to reason, the more of them there are, the less painful the contractions. When you’re immersed in the deep water of a body temperature birth pool, not only does it encourage Endorphin production but has a productive effect on your Oxytocin levels as well. This may also be because the illusion of space you feel by floating in the pool, creates a sense of solitude. That increase of Oxytocin often means a baby will be born within a couple of hours after getting in to the pool (if the mum enters it at the right time of course.)
Hospitals can be very particular about when they will ‘allow’ a woman into the water, because there is a belief getting in too soon will slow the contractions. Once the contractions have reached a regular pattern and are increasing in strength, a birth pool is unlikely to stop the flow. If it does, you can always get out for a while.
Birth gurus such as Michel Odent and Janet Balaskas have written extensively on this fascinating subject.
Liked Because:
- No risks to mum or baby.
- Can reduce the length of labour.
- Mum is less likely to need other forms of pain relief or intervention.
- Mum will feel more buoyant and able to change positions more easily.
- Can reduce the risks of tears to the perineum.
- Leads to a more ‘hands-off’ birth as it is not so easy to touch the mother when she is in the pool.
Disliked Because:
- Only recommended for low-risk births (although some delivery suites do have a birth pool option)
- May not enjoy the sensation of being in the water It can be very warm in the pool
Gas and air (Entenox)
Gas and air is made up of 50% oxygen and 50% nitrous oxide.
Hospitals usually pipe the gas into the delivery rooms, but it can also be provided in a cylinder for home births.
It is inhaled through a mouthpiece and for best results it needs to be sucked in at the beginning of the contraction. It works by making you feel very floaty as the contraction reaches its peak. It is not so much that it takes the pain away, you’ll just care less about it. Some of the more negative effects of the Gas and Air can be felt if you use it too early. Using it when labour is more advanced, could mean side effects aren’t felt as much. Liked Because: No risks to mum or baby Mum remains in control It can be used in any position and in conjunction with any other form of pain relief it is exhaled immediately so no lingering effects if mum decides she doesn’t like it.
Disliked Because:
Side effects can include
- dizziness and nausea, similar to having one alcoholic beverage too many!
- It can make mum very thirsty and her lips dry
- Can take a bit of practise to get it right
- Only available once she gets to hospital (unless you are booked with the Homebirth team who will have portable bottles).
Opiates
Depending on which hospital you’re in, you may be offered pethidine, meptid or diamorphine. All are forms of opiates and they are given via intra-muscular injection. They take about 20 minutes to work and act like a sedative, altering perception of pain and time, a bit like the gas and air, rather than an actual pain reliever.
Once administered it lasts up to four hours and usually you can have a couple of doses, depending on how long labour lasts.
Full disclosure – the opiates have some pretty major side effects (listed below) but they can work successfully, especially if the early/excitement phase has been long and the mother needs to rest. It can also help to relax her so successfully that if baby is in an awkward position, once the stomach muscles relax, it’s easier for the baby to turn. It’s also a big jump to go from gas and air to an epidural and this might provide a bit of down time before any decisions are made.
Liked Because:
- It can allow the mother to rest between contractions
- It can help a tense mother to relax allowing baby to move into a less awkward position
- It can be administered by the midwife
Disliked Because:
- It crosses the placenta, so if administered too close to the baby being born it can cause feeding and breathing difficulties
- It can cause nausea and sickness (sometimes it is administered with an anti-emetic)
- Mum cannot use the birth pool unless it has been 4 hours since the injection was given
- If it causes mum to fall asleep in between contractions she might only wake again at the peak of the contraction and be unable to help herself cope with it
- If mum doesn’t like it, there is nothing she can do about it until it has left her system
Epidural
The mighty epidural is often seen as the Holy Grail of pain relief and, if it works, it will take away the pain completely however it doesn’t take away the awareness of pressure in the vaginal area. However, this too has some pretty major side effects and because it cuts off the body’s communication system and the catheter acts as a barrier, it blocks the production of labour hormones which will slow labour down and possibly lead to further intervention. Nowadays there are such things as mobile epidurals or low dose epidurals because, in theory, the pain-relieving elements are there, but the complete numbing effect is not, so a woman is able to be more mobile. In reality, whilst I have seen some clients able to walk themselves to the toilet, despite being epiduraled up, far more women are likely to feel immobile. Midwives can be fairly uncomfortable about allowing a woman to mobilise with an epidural because the more the drug is topped up, the more like a traditional block it becomes and she becomes a ‘fall risk’ potentially causing injury to herself, her baby and maybe even the midwife who has to drag her back on to the bed! Finally, the lower dose and mobile epidurals have a higher concentration of opiates in their make-up, which we know crosses the placenta.
Liked Because:
- It can provide total pain relief It can be topped up if necessary It can allow a very tired or frightened mother to rest
- It lowers blood pressure (which is good if yours is high)
Disliked Because:
- It is a fairly complicated procedure and requires an anaesthetist to administer it. In other words, a mother can be desperate for one, but if there is no anaesthetist available there is no epidural.
- It might not work or may only provide a partial block.
- It takes about 20 minutes to work.
- It lowers blood pressure (which is not good if there’s nothing wrong with your blood pressure) To counteract this, a saline drip will be set up at the same time.
- A skin infection can develop at the epidural site.
- It can cause a fever in the mother.
- A catheter is required because a woman is often unable to feel if she needs the toilet or take herself there once the epidural is set up.
- It leads to an increased risk of assisted delivery because of the cascade of intervention and immobility of the mother.
- An epidural also changes the shape of the pelvic floor, making it very hard for the baby to turn against it.
- About 1% of women will suffer a dural tap (a leak in the spinal fluid) which can cause a severe and debilitating headache.
- It can lead to spinal injury and paralysis and in some cases death (very rare according to Reynolds, F., 1989)
Helpful Strategies
Your Partner
There are many other tools and techniques that can help with the lead up to and the process of labour – the most valuable of which is your partner! It doesn’t matter whether they are your romantic partner, your best friend, your mum, your sister or a doula, the same rules will apply. The beauty of hypnobirthing is you’ll be able to do it all by yourself. Whether you choose to listen to the downloads during your labour, or whether you choose to simply listen to music you find relaxing, you’ll be so subconsciously conditioned to enter a deep level of relaxation and focus, that you’ll be able to do it simply by closing your eyes and breathing. However, it will give you great comfort and an even greater level of relaxation knowing that your partner is there to support you should you find you struggle at any point. The Hodnett review (2002) found that when a mother feels supported they are more likely to feel safe and be able to cope much better with pain and everything that labour brings (hardly rocket science is it? Still nice to know they have done some research on it so we have evidence!!). In addition, a lot of the techniques we have discussed in this book can be hugely beneficial for any partner who’s feeling nervous about the prospect of their supporting role. Also vital to calm themselves down if they are feeling nervous during the birth as it is quite easy to ‘catch’ Adrenalin which would be detrimental to the birthing woman for obvious reasons.
Whether you are attending a course or if you are doing this online then I hope that this will help you and your birth support/partner …
Vital tips on how to enhance the hypnobirthing techniques and support you during labour:
- Reduce neocortex stimulation
The aim is to enable the mother to become as mammal-like and give birth as instinctively as possible. - Turning the lights off, not only makes her feel more private and less observed, it also encourages the body to produce melatonin which will make her feel sleepy and therefore more relaxed and it also encourages the release of oxytocin.
- It is very important to avoid asking her any questions, because she will have to think in order to reply.
- Offer her things instead, such as drinks, food, massages etc. and answer any questions the midwife asks on her behalf.
- Obviously, receiving permission for an internal examination will need to come from the mother herself, but answering questions on how long the contractions have been happening etc. is ideal.
Use of triggers
Her subconscious will have learnt to respond positively to certain smells, your touch, the familiar things around her, words and phrases you say to the mother whilst in labour, as long as they have been incorporated into her post-hypnotic suggestions and hypnobirthing practice.
Using them at appropriate times will enable her to sink even deeper into relaxation and feel calm, relaxed and safe wherever she is giving birth to her baby.
Remember these triggers are even more important when a birth is happening in a medical environment.
Environment
Make sure her environment is as ‘familiar’ as possible.
She needs to feel safe and protected at a subconscious level in order for her neocortex to switch off and her instinctive, mammalistic brain to take over.
Keep her fed and watered
She is about to embark on a very physical experience. It is absolutely impossible to do this without her energy levels being kept up.
Make sure she drinks and feed her throughout her labour. She may be able to eat more at the beginning of the process but as things get more established give her a chocolate button after each contraction or a spoonful of honey.
If she is using a birth pool or in and out of the bath and shower a lot, she will also need isotonic drinks to keep her electrolytes up.
Make sure she wees
Keep an idea on how much she is drinking and make sure she goes to the toilet regularly.
A full bladder is going to get in the way of the baby moving down the birth canal. If she finds it difficult to wee and she hasn’t been for a while, the midwives can use an in/out catheter to drain the urine. It is not painful and is far less invasive than a permanent one which she would need if having an epidural or caesarean.
Emotional stages of birth
You’re not going to have access to the cervix (nor are you likely to know what you’re feeling for) and even if you did, cervical dilation does not provide an accurate assessment of how close she is to having her baby. It is far more informative (combined with length and strength of contractions) to pay attention to her emotional moods.
The Excitement Stage relates to the latent/early stages of labour.
A woman in this stage is likely to be talkative, make eye contact and be excited because she has been waiting for an extended period of time for this to happen. Contractions are typically shorter and erratic at this time, and even if she has to close her eyes and breath through them she usually comes straight back to the room, once they have finished. This stage can last a long time and it is important that she rests and eats. Having some sort of project to focus on at this stage can act as a welcome distraction. You should match her mood.
After, what could be many hours, she will enter The Serious Stage, this is the equivalent of the established 1st stage of labour.
By this stage, the contractions are probably lasting 45 – 60 seconds and are possibly 3 – 5 minutes apart. This stage can also last many hours and she is likely to stop talking to enable her to concentrate on each contraction. She will want to move around more with each one and, in between, she is likely to want to rest. You should match her mood again, and at the same time encourage and support her with triggers, massage, words of reassurance and affirmations. At some point her contractions will increase in intensity and length. They will feel very close together and it is likely she will feel they are double-peaking. She is likely to show signs of Self-doubt, declaring she can’t do it any more, she has changed her mind about having her baby and if she is not already using pain relief she is likely to ask for it at this point. This stage is the equivalent of transition and is the final part of the first stage, just before her body starts pushing the baby out. Whereas you have matched her mood during the previous stages it is not a good idea to do so now! She will need extra encouragement and support and reminders she is so close to having her baby. It is worth noting that some hypnobirthing women are very quiet and extremely focused. It can be quite difficult in these circumstances for you to be able to tell where they are in the labour so just take your lead from them and match their mood.
Breathing and jaw
You can help a labouring mother to focus on her breathing which in turn will help trigger the relaxation response, by ‘modelling’ the type of breathing she should be doing. This works even better if it is something you have practiced together. Be mindful that the state of her jaw correlates directly with the muscles of the cervix. If her jaw is tight (as in she is clenching her teeth) then the cervix will find it harder to open. I like to tell people “If the mouth isn’t smiling, the cervix isn’t smiling either!” You can encourage her to relax her jaw by stroking her cheek, telling her or ‘modelling’ horse breathing i.e. fast exhalation of air through relaxed lips
B R A I N S
Remember to use them! It is a good idea to discuss what her plans are for labour beforehand and draw up a birth plan so whilst she is occupied during contractions you’ll have a fair idea of what she needs and wants and can advocate for her if she is unable. If interventions are suggested, during labour, ask your BRAIN questions to help you to clarify the situation. Remind the laboring woman that, as long as there is no emergency, she has time to decide or to wait and see what happens.
Take control
If she needs you to. Occasionally, at various points in her labour, it is quite possible that she may appear to have lost control and not be able to get control of her breathing. It’s normal, it happens, mostly as things are shifting up a gear but you don’t have to stand by feeling helpless. Firstly take a calming breath yourself and then ‘model’ how she should be breathing which is with focus on the exhalation.
Have a code word
It is very normal for a labouring woman to ask for pain relief or say she can’t do it at some point. It usually happens as she is transitioning from one stage of labour to another and is known as going through self-doubt, however, it can be very difficult to know if she really does want something stronger or she is just saying it because it helps. When I work with clients as their doula, I suggest the couple come up with a code word that has nothing whatsoever to do with labour. Ones that have been successful in the past have been ‘yellow’, ‘butterflies’ and even ‘peanut butter’! This way, you know she is being serious if she says the word but if she threatens to say the word or calls for a drug by name, she is asking for encouragement and support.
Just ‘be’
As a birth keeper or birth partner it can be very challenging to observe when a loved one is experiencing something so incredibly intense & physical. Our instinct is to step in and fix it. Well this can’t be fixed … it just has to happen and sometimes just being there for her to make eye contact with, just offering a hand to squeeze or a pair of shoulders to hang off of, is more than enough.
On another note, partners are great channellers of Oxytocin. If you’re with a friend or romantic partner during labour, a hug, a squeeze and loving eye contact can really encourage this super hormone to flood your system.
But there are two secret weapons that can be super helpful in labour because of their effectiveness at producing Oxytocin.
No 1. A pet! Preferably a dog, or a cat if you’re that way inclined (the jury is out regarding iguanas, goldfish or hamsters – but do let me know) A Japanese study reported that dog owners experienced a jaw-dropping 300% increase in oxytocin levels after spending half an hour with their dogs (Hills, 2019)
No 2. Sex! I know, I know – hard to believe that anyone could be even remotely interested in sex whilst in labour but Ina May is a great fan of an orgasm during labour as it is the ultimate Oxytocin releaser. Even if an actual orgasm seems slightly unrealistic, Oxytocin producing activities can certainly help.
Kissing, touching, stroking can all help but particularly effective is nipple stimulation (stroking not ‘tuning a radio’!) and clitoral stimulation. If you can’t face the idea of your partner touching your clitoris during labour – a doula colleague of mine suggests her clients get hold of a bullet vibrator. Small, discreet but effective! You can do all this privately and ask for space to explore this without disturbances. If you joining me ask me about the couple being induced … it’s a fabulous birth story …
Positions for Birth
G E T O F F Y O U R B A C K … I will consistently say this …
Women are not meant to be lying on their backs whilst giving birth.
When you’re upright and able to move as you choose, you create a staggering 28-30% more room in your pelvis which basically means you have given your baby a third more room to navigate its way through, to rotate and to descend. What’s not to love? In addition, in comparison to women who gave birth lying on their backs, those who gave birth in upright positions were: 25% less likely to have a forceps or vacuum-assisted birth 25% less likely to have an episiotomy 54% less likely to have abnormal foetal heart rate patters (Decker, 2018)
Contractions are more effective when in an upright position and some studies show that the first stage of labour (that’s the cervix opening bit) was on average 11/2 hrs shorter in the upright groups (WHO, 2014) and the second stage of labour (that’s the pushing bit) was shortened by about 34 minutes for women who remained in an upright position. They also experienced less pain and were less likely to need artificial oxytocin (Syntocinon) to speed labour up than those that gave birth while lying on their backs in a raised bed (Decker, 2018) So the moral of the story is GET OFF YOUR BACKS, PEOPLE!!! The only people who benefit from having a woman lying down in labour is those caring for her, because it is easier to see what is going on.
So what do you do if you’re having an epidural?
Well, you can still do a lot actually. The main factor in reducing the amount of assisted vaginal births with an epidural sited seems to be waiting until you feel a spontaneous urge to push, as opposed to being told to push because you’re fully dilated (Decker, 2018) but there is some evidence to suggest that being helped into a side-lying position with the lower leg remaining extended on the bed and the upper leg rested, flexed on a stirrup, also made a difference.
Using a peanut ball – basically a monkey nut shaped ball has been associated with decreasing the length of labour and a “significantly lower incidence of caesarean surgery” in those using an epidural (Tussey et al, 2015). Technically you’re not necessarily upright whilst using one of these things but depending on the positions you use, you’re creating more space in the pelvic capacity to allow your baby to make use of maximum room in the pelvis.





Massage
Massage can be hugely beneficial during labour as long as you want to be touched. If you like massage, it is definitely something you should practice in the lead up to birth so your partner feels confident in what he or she is doing. Don’t dismiss it if it is not something you particularly enjoy under usual circumstances because your needs can change in labour and sometimes counter pressure during particularly strong contractions or if you have an achey back can be just what you need. Different people are going to find different types of massage helpful.
So some people cannot stand soft stroking but it may be exactly what they need. They might find firm and rhythmic strokes, like the ones illustrated below, are more acceptable. The theory is that this gentle massage acts on the Gate Control Theory method by flooding the body with pleasant sensations so that the brain does not perceive the painful sensations as much because it is too busy concentrating on all the pleasant feelings instead. This sort of massage is fab for in between contractions to really help you to relax – so important because you want to be as relaxed as possible when the next one starts.
Gentle massage also helps to regulate your breathing which, as we know, stimulates the relaxation response. Gentle massage, especially when delivered by someone you love also triggers Oxytocin – Win Win!
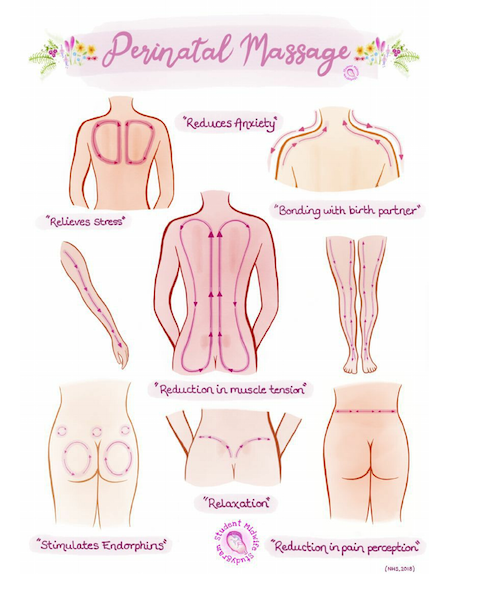
Here are some more examples of gentle massage techniques that can help to ground you, release adrenalin and get you out of your thinking brain.
Pressure wave
- Gentle sweep across the eyebrows.
- Move to the temples.
- Shoulders.
- Tops of arms.
- Forearms.
- Thighs.
- Calves.
- Top of feet and then sweep off.
- Gentle squeeze wherever your hands stop.
Head massage
- One hand on the back of her head and one hand on her forehead, slightly covering her eyes.
- Apply gentle pressure.
- Firmer, deeper massage acts on something called the Diffuse Noxious Inhibitory Control method of pain relief. The idea is that stimulation from intense, firm massage stimulates the brain to release endorphins which is going to mask the pain from contractions.
- It also helps to reduce cortisol and stress hormones and increase levels of dopamine and serotonin in the brain (Decker, 2018)
Firmer counter pressure can be done during contractions. Here are some examples:
Counter pressure
Apply pressure through the palms of your hand anywhere on her back where she is feeling discomfort. Use your body weight to increase pressure as opposed to your arms. Avoid leaning on her spine. Small of the back Using fingers or a massage ball, small circular movements with pressure in the small of her back.
Hip squeeze
Squeeze either side of the hips with heel of hands on hip bones to help the baby descend or move into a good position. By moving heel of hands slightly forward you can increase space at the front of her pelvis. The trick is to hold the squeeze for the length of the contraction – think of it as an upper body workout!
Sacral pressure
Placing your palms or hands on the sacral area of the lower back during a contraction. Many women find that this is a wonderful way of relieving pressure on the lower back during a contraction.
Shaking the apples
Between contractions – a vigorous rub down the mothers back, bottom and legs to release tension, release adrenaline, get the blood flowing and make her giggle!
A note to those doing the massage:
It is so important that you look after yourself during the labour process (that is not an excuse to do nothing, by the way) but the chances are, if she likes having massage, you could be doing it for a long, long time.
Make sure you’re in a good supported position as much as possible so as not to cause unnecessary muscle tension etc.
Make sure you wear comfortable clothes and, as make sure you drink and eat to keep your strength up.
You’re going to be no good to her if you pass out from dehydration and lack of energy
Perineal Massage
So yup lets put this topic out there .. some of you will pull funny faces, some will outright say nope not going there … some will sort of know what it is because they’ve chatted to their friends or have come along to my pregnancy yoga classes where I talk about vaginas within minutes of being in the class …
This is important … a Cochrane review showed that perineal massage undertaken by the woman as little as once or twice a week from 35 weeks of pregnancy reduced the likelihood of perineal trauma (mainly episiotomies) and ongoing perineal pain (Cochrane.org 2013)
There is a leaflet on how to do this leaflet perineal mass
The perineum is the area of tissue between your vagina and anus and it connects with the muscles of the pelvic floor – a hammock of muscles with supports your pelvic organs, such as your bladder and bowels.
Perineal massage is a way of preparing your perineum to stretch more easily during childbirth but it also helps you to make a mental connection between your head and that part of your body. So important in Western culture where the vulva and vagina are not often talked about, meaning that many women are terrified about the prospect of the baby’s head being born. In reality, the perineum can easily accommodate a baby’s head, due to the muscles in that area being ‘concertinaed’ over each other. Combined with the powerful hormones present during birth, they stretch apart under the pressure of the baby’s head, allowing the head to be eased out. As the baby’s head crowns, an intense stinging sensation can be felt (unhelpfully known as The Ring of Fire) which firstly lets you know that your baby is about to be born and secondly actually helps protect the perineum because it encourages you to bring your legs closer together to reduce any extra stretch on the area. The rocking of the baby’s head on the perineum as it crowns, creates more Oxytocin which is essential for the release of the placenta and bonding between you and your baby.
You can start perineal massage anytime from 34 weeks of your pregnancy and antenatal perineal massage can also help with your recovery after birth.
I’m going to share a couple of ways to do this however I am a great believer that you really don’t need any lubricant or oil however I shall share both ways.
Here’s how to do it:
Comfortable Positions:
Be in a place where you feel safe, secure, calm and where you won’t be interrupted
Propped up with pillows on a bed or sofa with your knees bent out and supported Resting your back in the bath with one leg on the side, then change legs
Standing under a warm shower with one leg on a stool, then change legs
Technique:
Use a small amount of unscented, organic oil such as olive oil, grape seed, or K-Y Jelly or look at The Birthlight way below which doesn’t use anything.
- Don’t use synthetic oil such as baby oil or Vaseline.
- Make sure your hands are clean before you begin.
- You might find it easier to use a mirror for the first few tries.
- Place one or both thumbs on and just within the back wall of your vagina, resting one or both forefingers on your buttocks.
- Pressing down a little towards your rectum, gently massage by moving your thumb(s) and forefinger(s) together upwards and outwards then back again, in a rhythmic ‘U’ shaped movement.
- You’re aiming to massage the area inside your vagina, rather than the skin on the outside – although you might feel a stretching sensation on the skin on the outside.
- Focus on relaxing your perineum as much as possible during the massage.
- It can last as long you wish, but aim for around five minutes at a time.
- For benefit, every or every other day is recommended.
- Do not do the perineal massage if you have a vaginal infection or thrush, upon advice from your care provider or if you experiencing pain.
- If you do tear or require stitches make sure you drink lots of water to dilute your urine to prevent it being too acidic.
- When you wee, it can help to pour warm water over your perineum as you do so, or maybe even wee when you’re in the shower or in the bath.
- Avoid wearing period sanitary towels that are plastic backed (stick to the actual maternity pads instead) as they can make the area sweat.
- There are many soothing products on the market you can buy to help aid your recovery, or you can even keep some maternity pads in the freezer so they are cool and soothing when held against the area.
***** The Birthlight Way ******
- Find a comfortable relaxed position

Birth Plans or Birth Wishes?
To birth plan or not to birth plan?
Birth plans or birth wishes???
I remember having a doula client when I first started who had ‘laminated” her birth plan and colour coded it. There were some negative comments from one of the midwives supporting her and I remember levelling my gaze on her and she went very quiet. Similarly she had a comment to make when transferring in from a successful Homebirth due to a retained placenta and the comment was “it’s a hypnobirthing patient” said in such a derogatory tone and once again I just levelled my gaze at her and she dropped her eyes knowing she had been overheard. Let’s just say that anytime that particular midwife came into a clients home I was on my guard and very protective of the clients space.
Who cares how you present your birth wishes … they are your thoughts on how you would like to journey to meet your baby and welcome them into your loving arms. This should be read and your choices acknowledged.
It shows what is important to you and, regardless of how your baby is born, there will be elements that can be transferred from ideal birth to actual birth, enabling you to feel that you have been listened to and heard!
Taking the time to write it can also help you to consolidate everything you have read and put it in to context.
Try the exercise on the following page and fill in all the things you have read about which you think you’ll find useful before, during and after your labour. This will then help you to formulate your ideas.
Some examples might include:
Before the birth
Listen to my downloads
Plan my nest
Excited Mama
Watch box sets on TV
The birth
Instinctive pushing
After the birth
Lots of cuddles
When writing your goals, it is important to focus on what you want to feel about the birth when you look back at it, rather than having a specific type of birth or giving birth in a specific place. That way, if things should go in a different direction from what you had originally planned, you can still, rightfully, feel like you smashed it!
Your Last Days of Pregnancy
Due dates.
Many a conversation has been had about this and wouldn’t it be wonderful if we knew exactly when we would go into labour? Would it take away the uncertainty, the unnecessary conversations around induction, the constant pestering from family, friends and colleagues of “is the baby here yet?” In previous generations we knew that we could be having a spring baby or a summer baby again nothing to set in stone.
From the moment we are given that due date everything becomes focused on that and any conversations are centred about what happens before or after that date.
We should always remember that our baby is full term at 42 weeks according to the WHO guidelines and therefore anything that may be considered should be discussed and may be chosen after this point.
When you go for your booking in appointment with the midwife she will calculate your due date according to something called Nagele’s Rule. Nagele was a chap who in 1812 came up with a concept based on the work of a professor from the Netherlands, Herman Boerhaave which said that the due date can be figured out by adding 7 days to the last period and then adding 9 months which is roughly 280 days (Decker R. 2019). However neither Professor made it clear whether their intention was to add 7 days to the first day of the last menstrual period or the last day. In the 1900s it was written into text first day which is why that method, despite being based on no evidence whatsoever (and perhaps not even what Naegele intended) is what is used today. The problems don’t stop there. The rule, as it stands, is based on every woman having a 28 day cycle and ovulating and conceiving on day 14 – which rules out about half the menstruating population.
Some studies have shown that, in reality, it is far more accurate for a woman to give birth on or around 40 weeks of pregnancy plus 5 days. Around 50% of women will have given birth by this stage and the other 50% will not. A pretty accurate predictor as to whether you can expect a longer pregnancy is to look at your mother and/or sister. If they had pregnancies going beyond 42 weeks, there is a pretty good chance you will too. Remember though, just because a pregnancy might last 44 weeks or so on paper, that is counting from the first day of the last period – with women who have longer cycles, irregular cycles or ovulate towards the end of their cycle, the actual length of pregnancy is likely to be between 40 and 42 weeks (Decker R, 2019.) Things you can do to help with your mindset over this time is, if it’s not too late, give people a due month when they ask you to try and cut down on the amount of people who are likely to bug you as you wait (patiently!) for your baby’s arrival. The other thing is to fill your diary for at least the two weeks past the date you have been given – if you’re anything like the majority of my clients, you’ll have the due date highlighted in your diary and a blank schedule for the following two weeks due to the fact your baby will have arrived. In that time, if you can, treat yourself by doing the things you love to do. If you have a partner, schedule in some special time with them as it is unlikely you’ll be able to do things a deux for a little while after. Spend some quality time with friends or family, go to the cinema, rest and watch old movies. I know it sounds clichéd but you’ll never get the opportunity to repeat this
time if this is your first baby, or spend time alone with your existing child if this is a subsequent pregnancy. Take advantage of it. Remember, your baby is not a piece of fruit that needs to be plucked from a tree – when it is ripe enough, it will fall on its own. Natural methods of induction Despite all I have said above, it is quite normal to want to try and speed things up and there are various different methods out there that are said to be effective in sending an overdue mama into labour. In reality, most of them are just old wives tales and you can work your way down the whole list, doing each and every one of them several times over – but if your baby is not ready to be born, it will not make the blindest bit of difference. However, there are a couple that are evidence based so might just be worth a try: Dates – some trials have found eating 6 dates a day from 36 weeks of pregnancy may increase cervical ripening, reduce the need for
medical labour induction or augmentation and one small study found a positive effect on postpartum blood loss (Decker. R, 2017). By the way, don’t do this if you have been diagnosed with gestational diabetes. Nipple stimulation – we know nipple stimulation produces oxytocin and there is some evidence to suggest stimulating the breasts either by hand or by a pump can be successful in sending a heavily pregnant woman into labour. In studies where women were encouraged to stimulate their breasts from 38 weeks, there was an increase in cervical ripeness, less need for caesareans and shorter labours (Decker. R, 2017). However, this method can lead to hyperstimulation of the uterus so should only be done in women with low risk pregnancies. Anecdotally, many women try reflexology and acupuncture to help them go into labour. A Cochrane review (Smith et al., 2017) said although there is some evidence to suggest these methods may help to
ripen the cervix, more conclusive studies are needed. So, in conclusion, patience is definitely the best path – (*ducks as several items are thrown in my direction). I have been known to send this article to clients in the past as I think it sums up that period of waiting for your baby, perfectly: The Last Days of Pregnancy: A Place of In-Between by Jana Studelska She’s curled up on the couch, waiting, a ball of baby and emotions. A scrambled pile of books on pregnancy, labour, baby names, breastfeeding…not one more word can be absorbed. The birth supplies are loaded in a laundry basket, ready for action. The freezer is filled with meals, the car seat installed, the camera charged. It’s time to hurry up…. and wait. Not a comfortable place to be, but wholly necessary. The last days of pregnancy— sometimes stretching to agonizing weeks—are a distinct place, time, event, stage. It is
a time of in between. Neither here nor there. Your old self and your new self, balanced on the edge of a pregnancy. One foot in your old world, one foot in a new world. Shouldn’t there be a word for this state of being, describing the time and place where mothers linger, waiting to be called forward? Germans have a word, zwischen, which means between. I’ve co-opted that word for my own obstetrical uses. When I sense the discomfort and tension of late pregnancy in my clients, I suggest that they are now in The Time of Zwischen. The time of in-between, where the opening begins. Giving it a name gives it dimension, an experience closer to wonder than endurance. I tell these beautiful, round, swollen, weepy women to go with it and be okay there. Feel it, think it, don’t push it away. Write it down, sing really loudly when no one else is home, go commune with nature, or crawl into a loved ones lap so they can rub your head until you feel better. I tell their men to let go of their
worry; this is an early sign of labour. I encourage them to sequester themselves if they need space, to go out if they need distraction, to enjoy the last hours of this life-as-they-now-know-it. I try to give them permission to follow the instinctual gravitational pulls that are at work within them, just as real and necessary as labour. The discomforts of late pregnancy are easy to Google: painful pelvis, squished bladder, swollen ankles, leaky nipples, weight unevenly distributed in a girth that makes scratching an itch at ankle level a feat of flexibility. “You might find yourself teary and exhausted,” says one website, “but your baby is coming soon!” Cheer up, sweetie, you’re having a baby. More messaging that what is going on is incidental and insignificant. What we don’t have is reverence or relevance—or even a working understanding of the vulnerability and openness a woman experiences at this time. Our language and culture fails us. This surely explains why many women neonatal team, a woman must go to the place between this world and the next, to that thin membrane between here and there. To the place where life comes from, to the mystery, in order to reach over to bring forth the child that is hers. The heroic tales of Odysseus are with us, each ordinary day. This round woman is not going into battle, but she is going to the edge of her being where every resource she has will be called on to assist in this journey. We need time and space to prepare for that journey. And somewhere, deep inside us, at a primal level, our cells and hormones and mind and soul know this, and begin the work with or without our awareness. I call out Zwischen in prenatals as a way of offering comfort and, also, as a way of offering protection. I see how simple it is to exploit and abuse this time. A scheduled induction is seductive, promising a sense of control. Fearful and confused family can trigger a crisis of confidence. We’re not a culture that waits for anything, nor are we believers in normal birth; waiting for a baby can feel like insanity. Giving this a name points her toward listening and developing her own intuition. That, in turn, is a powerful training ground for motherhood.
Diosi, Dani. Hypnobirthing: Breathing in Short Pants . Birthing Awareness Publishing. Kindle Edition.
Diosi, Dani. Hypnobirthing: Breathing in Short Pants . Birthing Awareness Publishing. Kindle Edition.
Diosi, Dani. Hypnobirthing: Breathing in Short Pants . Birthing Awareness Publishing. Kindle Edition.
Let’s address the EPISIOTOMY you do not have to have one